The 51A209 form is a Massachusetts state tax form that is used to report the sale of capital assets. This form must be filed by taxpayers who have sold any property or assets that are classified as capital assets, such as stocks, bonds, and real estate. The information reported on the 51A209 form will help the Massachusetts Department of Revenue calculate the capital gains and losses resulting from the sale. Taxpayers who file this form should review it carefully to ensure that all necessary information has been included.
| Question | Answer |
|---|---|
| Form Name | 51A209 Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | refund kentucky form, refund kentucky get, refund kentucky paid, refund kentucky issued |

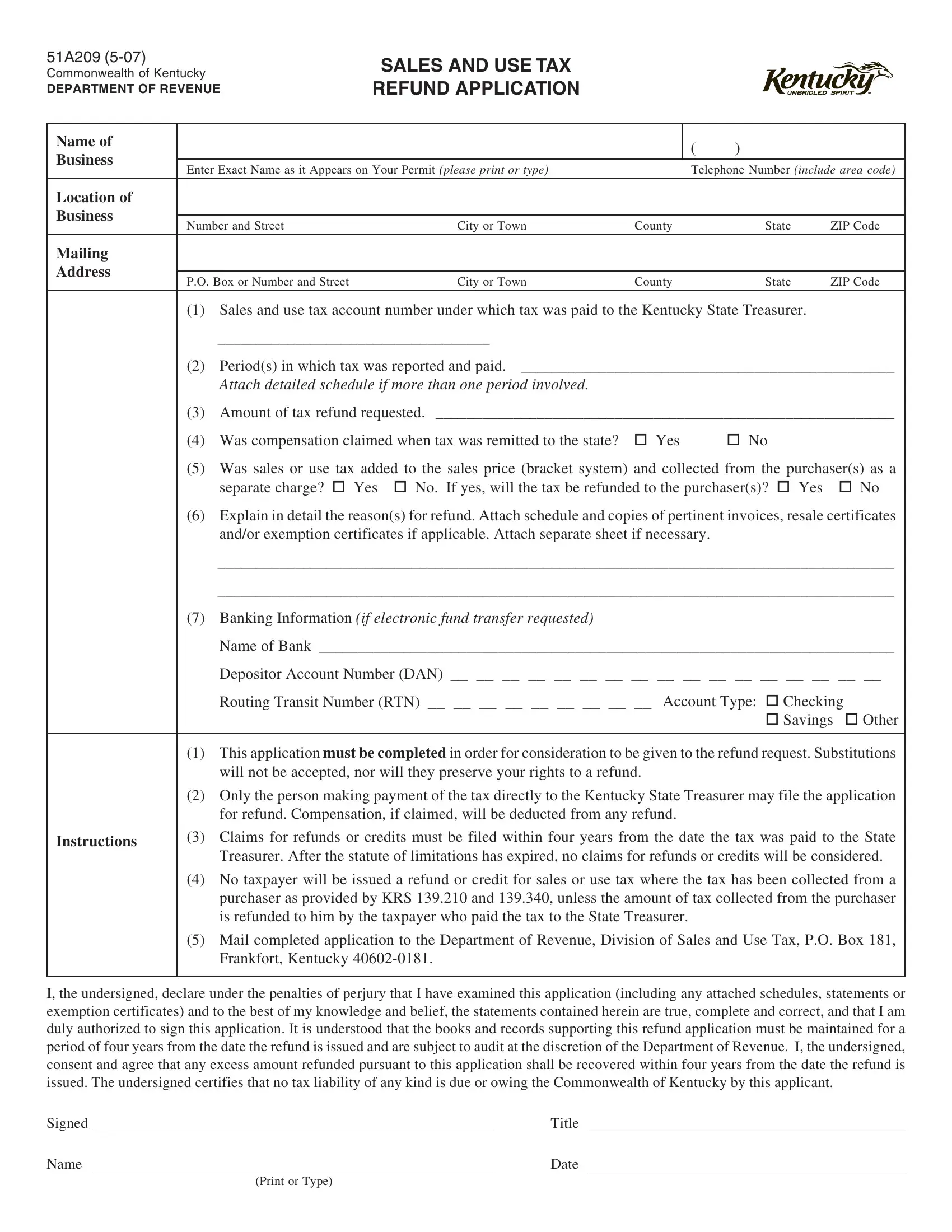
51A209
Commonwealth of Kentucky
DEPARTMENT OF REVENUE
SALES AND USE TAX REFUND APPLICATION
Name of |
|
|
|
|
|
( |
) |
|
|
|
Business |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
Enter Exact Name as it Appears on Your Permit (please print or type) |
|
Telephone Number (include area code) |
||||||||
|
|
|||||||||
Location of |
|
|
|
|
|
|
|
|
|
|
Business |
|
|
|
|
|
|
|
|
|
|
Number and Street |
|
City or Town |
County |
State |
ZIP Code |
|||||
|
|
|||||||||
Mailing |
|
|
|
|
|
|
|
|
|
|
Address |
|
|
|
|
|
|
|
|
|
|
P.O. Box or Number and Street |
|
City or Town |
County |
State |
ZIP Code |
|||||
|
|
|||||||||
|
(1) |
Sales and use tax account number under which tax was paid to the Kentucky State Treasurer. |
|
|
||||||
|
|
___________________________________ |
|
|
|
|
|
|
||
|
(2) |
Period(s) in which tax was reported and paid. ________________________________________________ |
||||||||
|
|
Attach detailed schedule if more than one period involved. |
|
|
|
|
|
|
||
|
(3) |
Amount of tax refund requested. ___________________________________________________________ |
||||||||
|
(4) |
Was compensation claimed when tax was remitted to the state? |
Yes |
No |
|
|
|
|||
|
(5) |
Was sales or use tax added to the sales price (bracket system) and collected from the purchaser(s) as a |
||||||||
|
|
separate charge? |
Yes |
No. If yes, will the tax be refunded to the purchaser(s)? |
Yes |
|
No |
|||
|
(6) |
Explain in detail the reason(s) for refund. Attach schedule and copies of pertinent invoices, resale certificates |
||||||||
|
|
and/or exemption certificates if applicable. Attach separate sheet if necessary. |
|
|
|
|
||||
|
|
_______________________________________________________________________________________ |
||||||||
|
|
_______________________________________________________________________________________ |
||||||||
|
(7) |
Banking Information (if electronic fund transfer requested) |
|
|
|
|
|
|
||
|
|
Name of Bank __________________________________________________________________________ |
||||||||
|
|
Depositor Account Number (DAN) __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ |
||||||||
|
|
Routing Transit Number (RTN) __ __ __ __ __ __ __ __ __ Account Type: |
Checking |
|
||||||
|
|
|
|
|
|
|
|
Savings |
Other |
|
|
|
|
||||||||
|
(1) |
This application must be completed in order for consideration to be given to the refund request. Substitutions |
||||||||
|
|
will not be accepted, nor will they preserve your rights to a refund. |
|
|
|
|
||||
|
(2) |
Only the person making payment of the tax directly to the Kentucky State Treasurer may file the application |
||||||||
|
|
for refund. Compensation, if claimed, will be deducted from any refund. |
|
|
|
|
||||
Instructions |
(3) |
Claims for refunds or credits must be filed within four years from the date the tax was paid to the State |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Treasurer. After the statute of limitations has expired, no claims for refunds or credits will be considered. |
||||||||
|
(4) |
No taxpayer will be issued a refund or credit for sales or use tax where the tax has been collected from a |
||||||||
|
|
purchaser as provided by KRS 139.210 and 139.340, unless the amount of tax collected from the purchaser |
||||||||
|
|
is refunded to him by the taxpayer who paid the tax to the State Treasurer. |
|
|
|
|
||||
|
(5) |
Mail completed application to the Department of Revenue, Division of Sales and Use Tax, P.O. Box 181, |
||||||||
|
|
Frankfort, Kentucky |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
I, the undersigned, declare under the penalties of perjury that I have examined this application (including any attached schedules, statements or exemption certificates) and to the best of my knowledge and belief, the statements contained herein are true, complete and correct, and that I am duly authorized to sign this application. It is understood that the books and records supporting this refund application must be maintained for a period of four years from the date the refund is issued and are subject to audit at the discretion of the Department of Revenue. I, the undersigned, consent and agree that any excess amount refunded pursuant to this application shall be recovered within four years from the date the refund is issued. The undersigned certifies that no tax liability of any kind is due or owing the Commonwealth of Kentucky by this applicant.
Signed |
|
Title |
Name |
|
Date |
(Print or Type)