If you are a business owner who needs to change the address on your BBB listing, you can use this form to make the changes. Be sure to provide complete and accurate information so that your listing can be updated as quickly as possible. Note that there may be a delay in updating your listing if incorrect or incomplete information is provided. Thank you for your cooperation!
| Question | Answer |
|---|---|
| Form Name | Bbs Address Change Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | bbs form request, bbs replacement license, bbs change, ca bbs address |
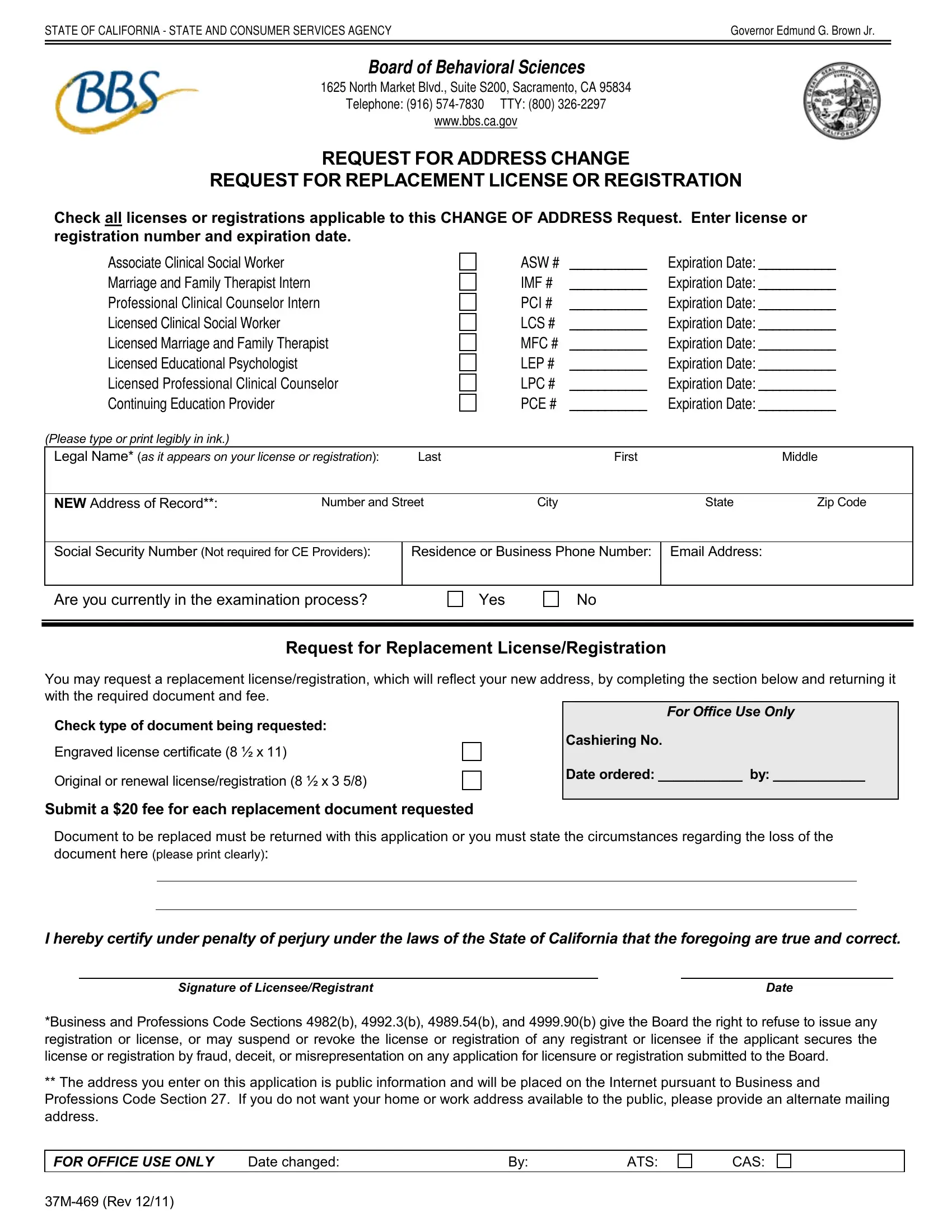
STATE OF CALIFORNIA - STATE AND CONSUMER SERVICES AGENCY |
Governor Edmund G. Brown Jr. |
BOARD OF BEHAVIORAL SCIENCES
1625 North Market Blvd., Suite S200, Sacramento, CA 95834
Telephone: (916)
www.bbs.ca.gov
REQUEST FOR ADDRESS CHANGE
REQUEST FOR REPLACEMENT LICENSE OR REGISTRATION
Check all licenses or registrations applicable to this CHANGE OF ADDRESS Request. Enter license or registration number and expiration date.
Associate Clinical Social Worker
Marriage and Family Therapist Intern
Professional Clinical Counselor Intern
Licensed Clinical Social Worker
Licensed Marriage and Family Therapist
Licensed Educational Psychologist
Licensed Professional Clinical Counselor
Continuing Education Provider
(Please type or print legibly in ink.)
ASW # |
___________ |
Expiration Date: ___________ |
IMF # |
___________ |
Expiration Date: ___________ |
PCI # |
___________ |
Expiration Date: ___________ |
LCS # |
___________ |
Expiration Date: ___________ |
MFC # |
___________ |
Expiration Date: ___________ |
LEP # |
___________ |
Expiration Date: ___________ |
LPC # |
___________ |
Expiration Date: ___________ |
PCE # |
___________ |
Expiration Date: ___________ |
Legal Name* (as it appears on your license or registration): |
Last |
First |
|
Middle |
|
|
|
|
|
|
|
NEW Address of Record**: |
Number and Street |
City |
State |
Zip Code |
|
|
|
|
|
||
Social Security Number (Not required for CE Providers): |
Residence or Business Phone Number: |
Email Address: |
|
||
|
|
|
|
|
|
Are you currently in the examination process?
Yes
No
Request for Replacement License/Registration
You may request a replacement license/registration, which will reflect your new address, by completing the section below and returning it with the required document and fee.
Check type of document being requested:
Engraved license certificate (8 ½ x 11)
Original or renewal license/registration (8 ½ x 3 5/8)
For Office Use Only
Cashiering No.
Date ordered: ___________ by: ____________
Submit a $20 fee for each replacement document requested
Document to be replaced must be returned with this application or you must state the circumstances regarding the loss of the
document here (please print clearly):
I hereby certify under penalty of perjury under the laws of the State of California that the foregoing are true and correct.
Signature of Licensee/Registrant |
Date |
*Business and Professions Code Sections 4982(b), 4992.3(b), 4989.54(b), and 4999.90(b) give the Board the right to refuse to issue any registration or license, or may suspend or revoke the license or registration of any registrant or licensee if the applicant secures the license or registration by fraud, deceit, or misrepresentation on any application for licensure or registration submitted to the Board.
**The address you enter on this application is public information and will be placed on the Internet pursuant to Business and Professions Code Section 27. If you do not want your home or work address available to the public, please provide an alternate mailing address.
FOR OFFICE USE ONLY |
Date changed: |
By: |
ATS: |
CAS: