
With the online tool for PDF editing by FormsPal, it is easy to fill out or edit DHS right here and now. To retain our tool on the forefront of efficiency, we strive to put into action user-driven capabilities and enhancements regularly. We are routinely looking for suggestions - assist us with revampimg how you work with PDF documents. To begin your journey, consider these easy steps:
Step 1: Open the PDF file inside our tool by clicking the "Get Form Button" in the top section of this page.
Step 2: With our handy PDF editing tool, it is easy to do more than just fill in blanks. Express yourself and make your docs seem professional with custom textual content added in, or optimize the file's original content to perfection - all backed up by an ability to add any images and sign it off.
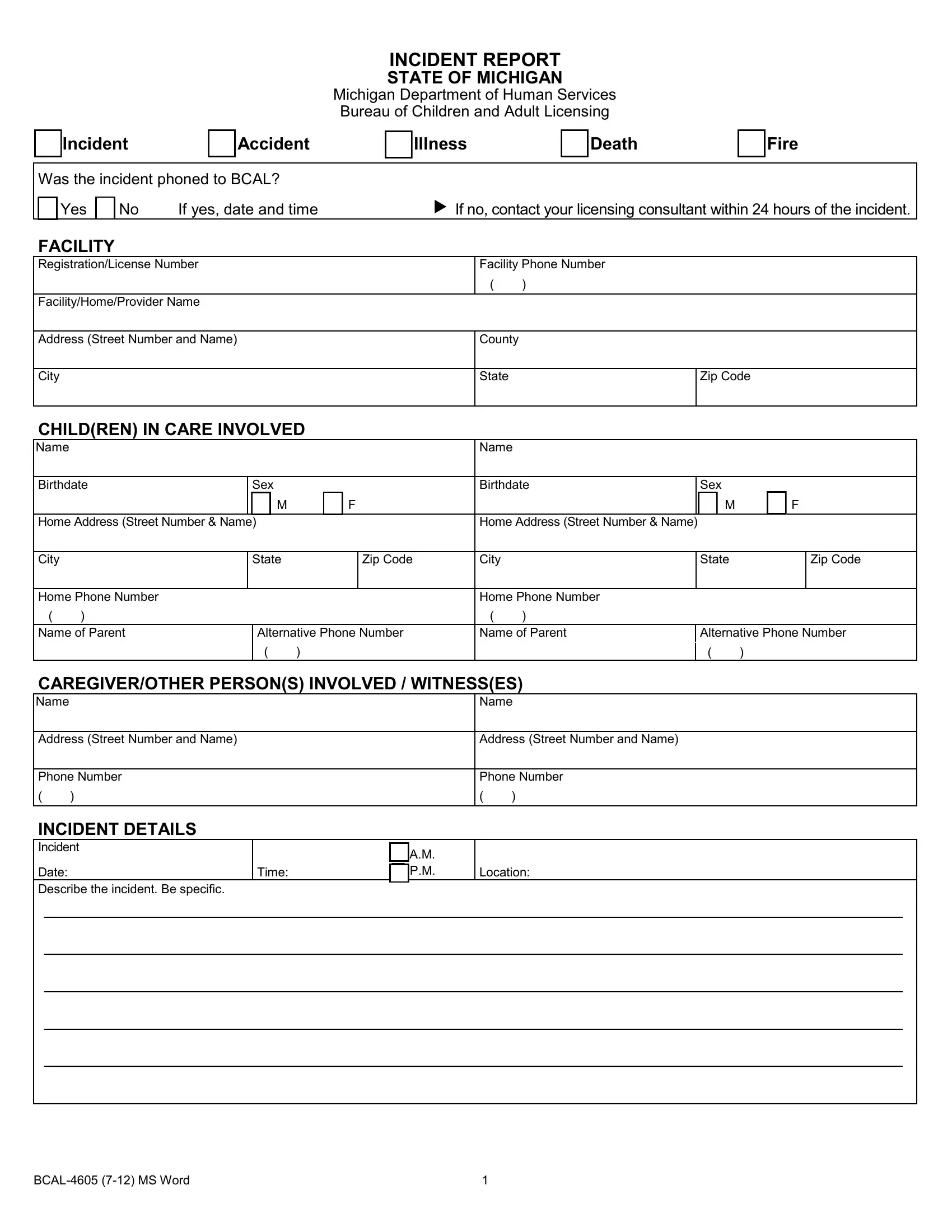
If you want to fill out this document, make sure that you enter the right information in each blank field:
1. You have to complete the DHS properly, therefore be mindful while filling in the sections containing these specific blanks:
2. Just after filling in the previous part, go on to the next stage and enter the necessary particulars in these fields - Home Address Street Number Name, Home Address Street Number Name, City, Home Phone Number, Name of Parent, State, Zip Code, City, State, Zip Code, Alternative Phone Number, Home Phone Number, Name of Parent, Alternative Phone Number, and CAREGIVEROTHER PERSONS INVOLVED .
3. Completing BCAL MS Word is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
4. The next section will require your involvement in the following parts: Was First Aid Given Yes No Illness, If yes when, Where Child Received Medical, By Whom, Phone Number of Treating Physician, Any Handicaps Health Problems or, If Fire Describe Damage, PERSONS NOTIFIED Law enforcement, Name of Person Notified, Notification Date, Notification, Time, AM PM, and AM PM. Make sure you type in all needed info to move forward.
5. This form needs to be completed by filling out this section. Further you will see an extensive listing of blanks that require appropriate details for your document submission to be accomplished: Signature of Person Completing, Signature of, Title, Title, AM PM, Date, and Date.
Be very mindful while completing Signature of Person Completing and Signature of, since this is where a lot of people make some mistakes.
Step 3: Once you've looked once again at the details in the fields, press "Done" to finalize your form at FormsPal. Right after registering a7-day free trial account here, you'll be able to download DHS or email it right away. The form will also be accessible from your personal account page with your changes. FormsPal guarantees your information privacy via a protected method that in no way records or distributes any kind of personal data provided. Be assured knowing your files are kept protected every time you use our editor!