
Working with PDF files online is definitely very easy using our PDF tool. You can fill out live of application here in a matter of minutes. Our development team is ceaselessly working to expand the editor and insure that it is even easier for users with its multiple functions. Discover an ceaselessly progressive experience today - check out and find out new possibilities as you go! With a few easy steps, you'll be able to begin your PDF journey:
Step 1: First of all, access the pdf tool by clicking the "Get Form Button" above on this webpage.
Step 2: With the help of our advanced PDF tool, you can do more than merely fill out blanks. Try all the functions and make your documents seem high-quality with custom textual content incorporated, or optimize the file's original input to perfection - all that backed up by an ability to incorporate just about any photos and sign the document off.
This PDF doc will need you to enter specific details; in order to guarantee accuracy, make sure you consider the following suggestions:
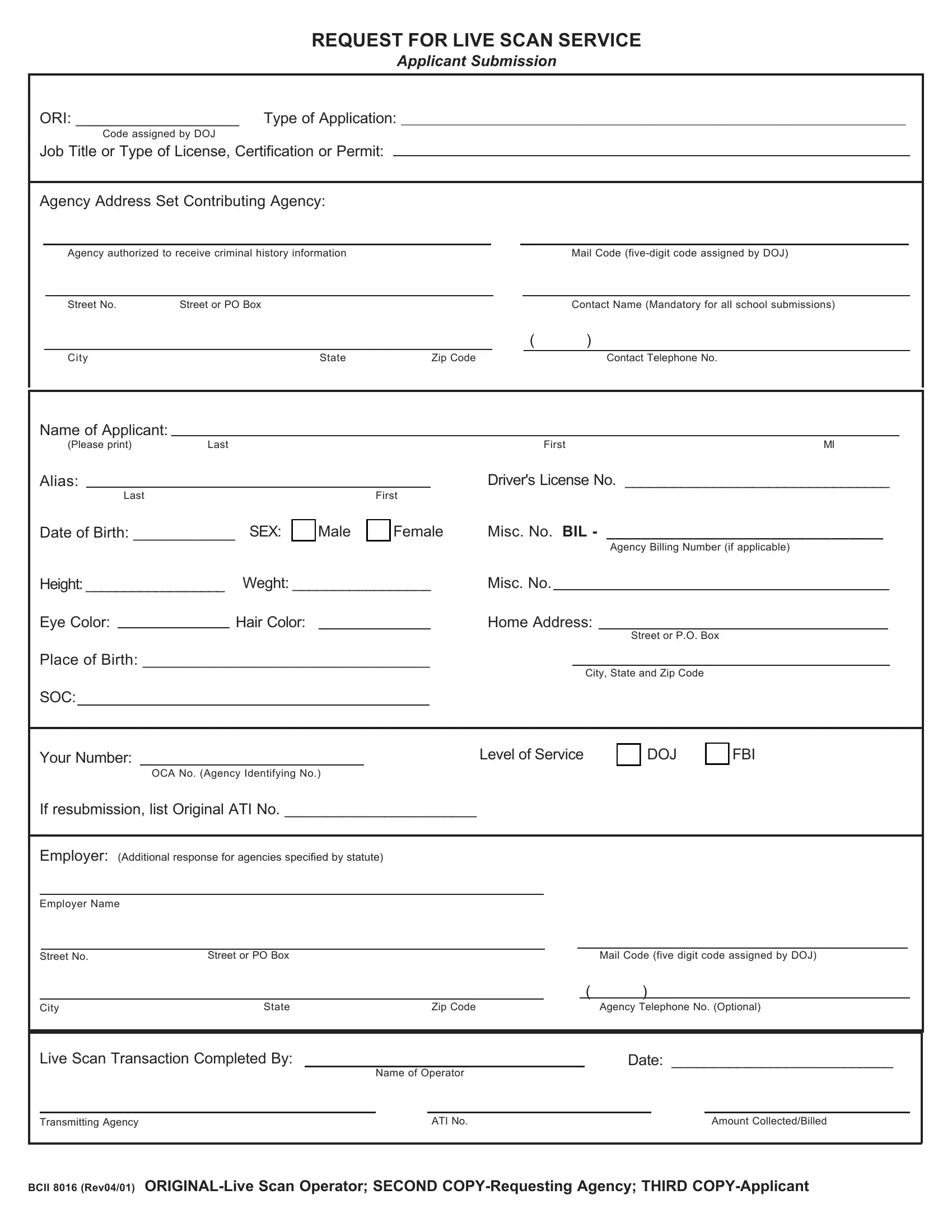
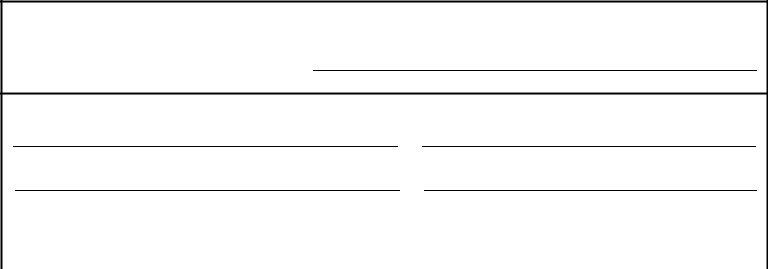
1. Fill out the live of application with a number of essential fields. Consider all of the important information and make sure nothing is neglected!
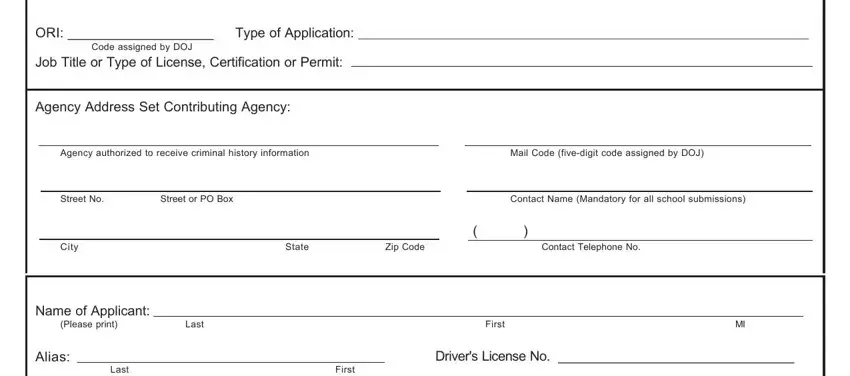
2. When this part is done, you need to insert the essential specifics in Date of Birth SEX, Male, Female, Misc No BIL , Agency Billing Number if applicable, Height Weght , Misc No, Eye Color, Hair Color, Home Address, Place of Birth , SOC, Street or PO Box, City State and Zip Code, and Your Number so you can progress to the third stage.
It is possible to make an error when completing your Eye Color, therefore be sure you go through it again before you decide to submit it.
3. Completing Live Scan Transaction Completed By, Date , Name of Operator, Transmitting Agency, ATI No, Amount CollectedBilled, and BCII Rev ORIGINALLive Scan is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
Step 3: Prior to submitting your file, ensure that all blank fields were filled out right. When you’re satisfied with it, click “Done." Create a free trial plan at FormsPal and acquire direct access to live of application - readily available in your FormsPal account page. We do not share the information that you provide whenever working with forms at FormsPal.