
bcbs claim form online can be filled in online very easily. Just try FormsPal PDF tool to finish the job quickly. The editor is consistently maintained by our staff, getting useful features and turning out to be more versatile. Should you be looking to start, here's what it will take:
Step 1: Click the "Get Form" button above. It will open up our tool so that you can start filling in your form.
Step 2: With this state-of-the-art PDF tool, you may accomplish more than simply complete forms. Edit away and make your docs seem professional with custom text put in, or modify the file's original content to excellence - all comes with the capability to incorporate just about any photos and sign the PDF off.
This document will require specific data to be filled out, so you must take some time to type in what's required:
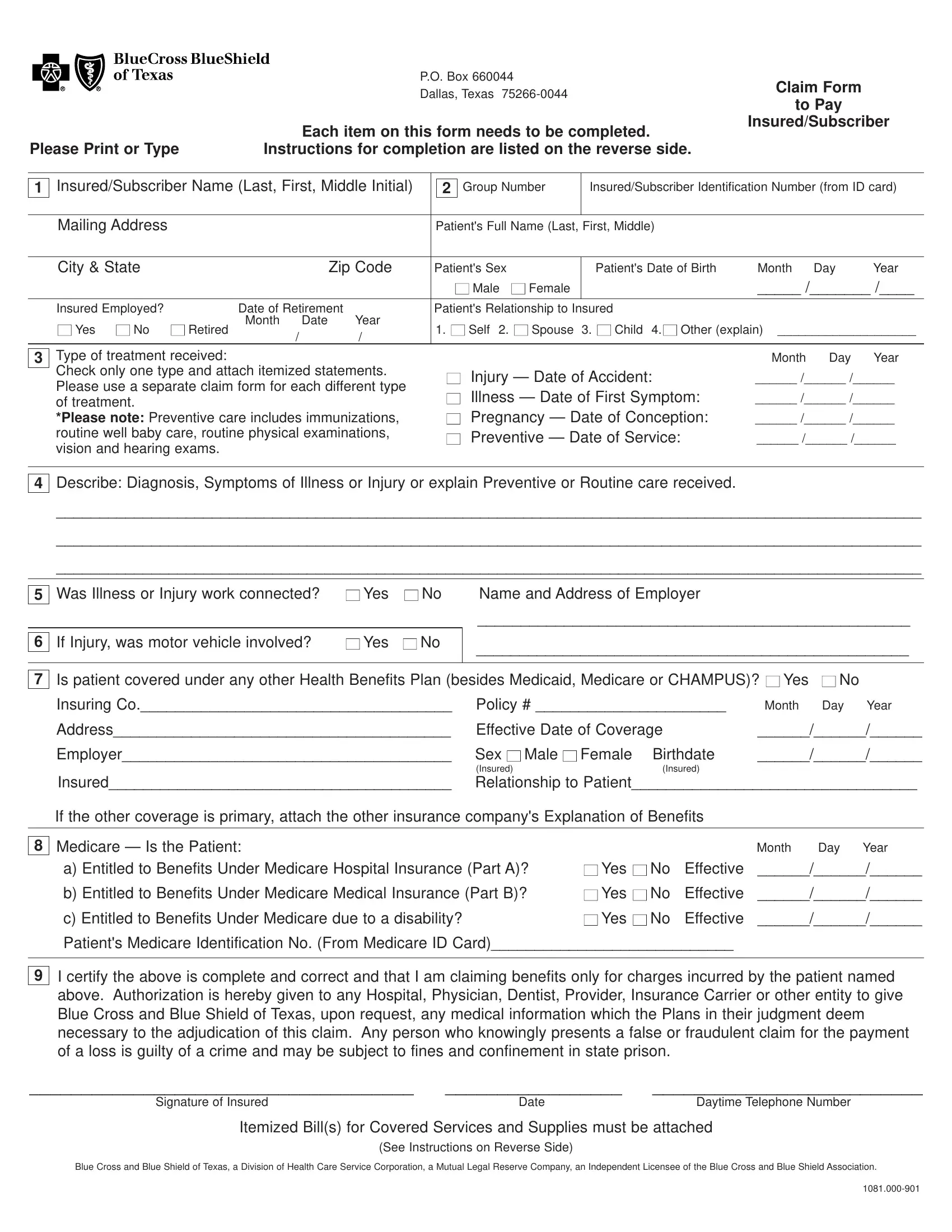
1. Start filling out the bcbs claim form online with a number of major fields. Consider all of the necessary information and make certain not a single thing omitted!
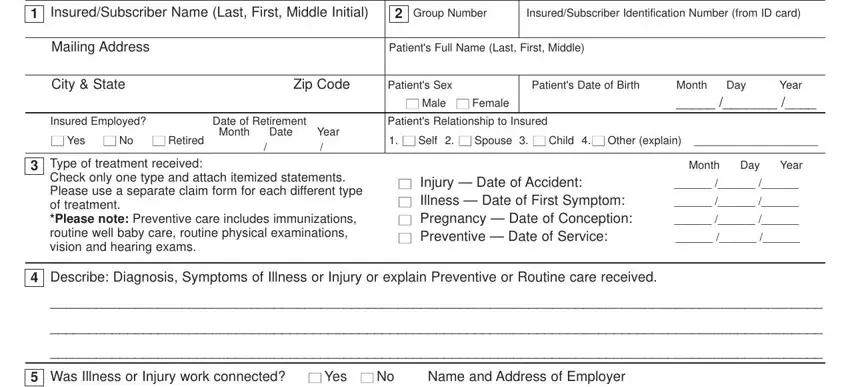
2. Soon after performing this section, go on to the subsequent stage and complete all required particulars in all these blanks - If Injury was motor vehicle, Yes , No, Is patient covered under any other, Yes , No, Insuring Co Policy , Month Day Year, Address, Employer, Insured, Effective Date of Coverage Sex , Female Birthdate, Male , and Insured.
People often get some things wrong when completing Yes in this section. Be sure you re-examine what you enter right here.
Step 3: Make sure that the information is accurate and then press "Done" to finish the project. Get hold of the bcbs claim form online the instant you register online for a 7-day free trial. Easily use the pdf file within your FormsPal account, with any edits and adjustments conveniently kept! FormsPal ensures your information privacy with a protected system that never saves or shares any type of sensitive information involved. Be assured knowing your paperwork are kept confidential each time you use our tools!