

If you need to fill out California Form Pm110, you won't need to download and install any software - simply try using our PDF editor. To keep our editor on the leading edge of convenience, we work to put into practice user-oriented capabilities and enhancements regularly. We're always looking for suggestions - play a vital part in reshaping PDF editing. It just takes just a few basic steps:
Step 1: Click on the "Get Form" button above. It will open up our tool so you could begin filling in your form.
Step 2: Using our advanced PDF editor, you could accomplish more than simply complete blank form fields. Edit away and make your forms seem high-quality with customized textual content put in, or modify the original input to excellence - all backed up by an ability to insert stunning photos and sign the document off.
When it comes to blank fields of this particular PDF, this is what you need to know:
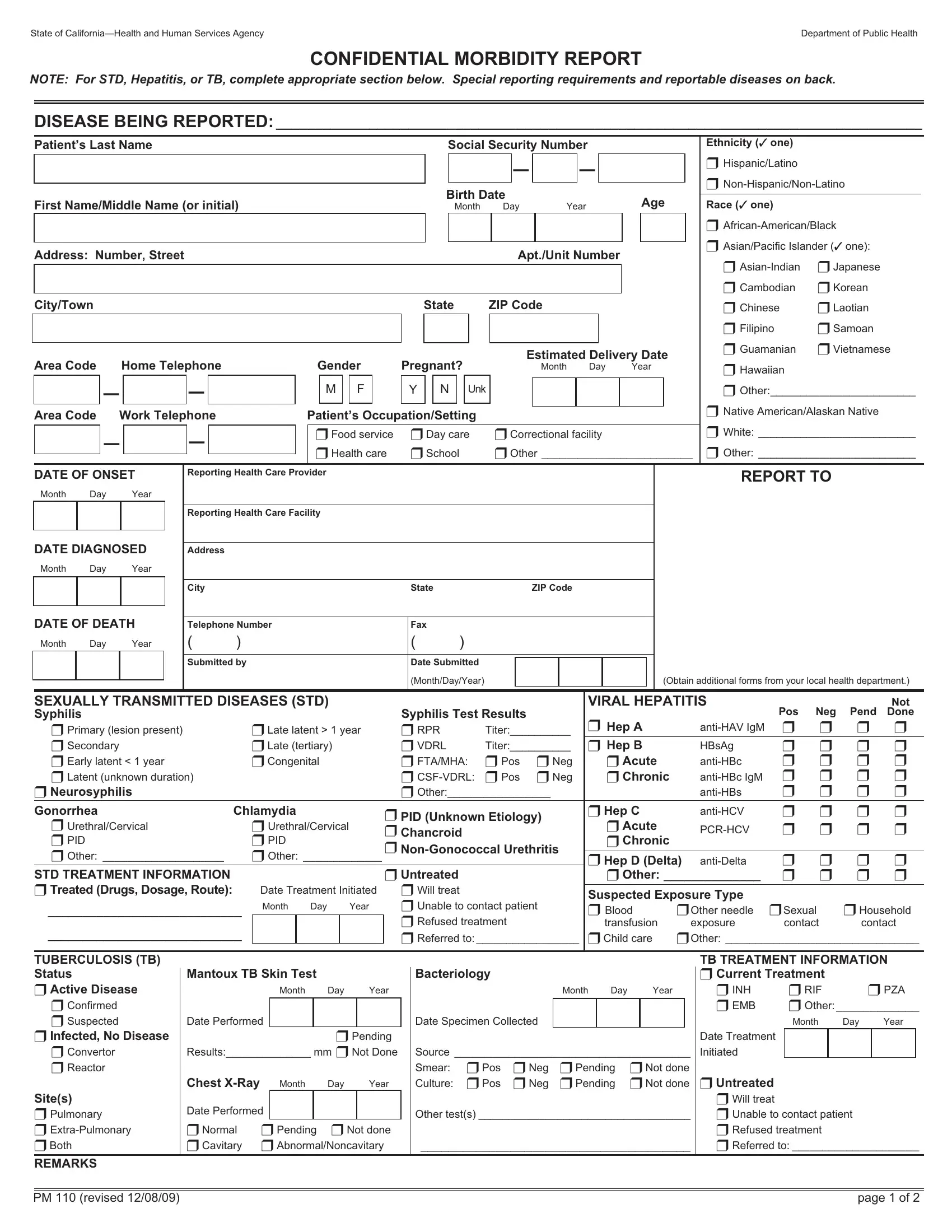
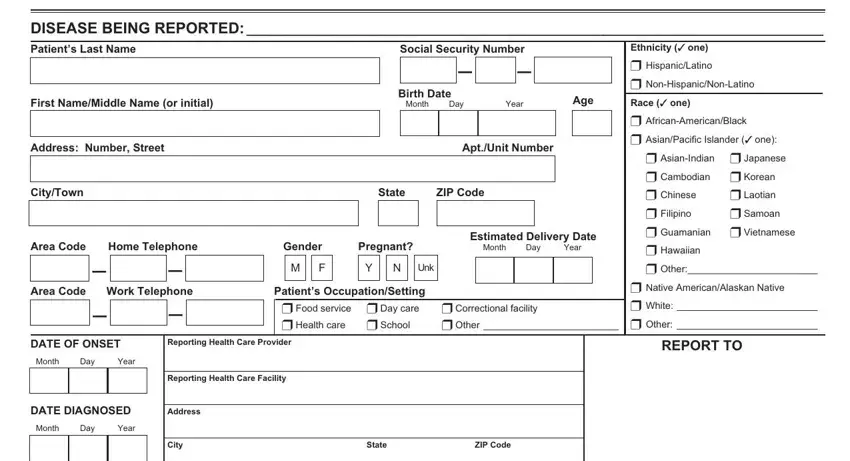
1. While completing the California Form Pm110, make sure to incorporate all needed blanks in their relevant part. This will help to facilitate the process, allowing for your information to be handled without delay and correctly.
2. Soon after completing the previous part, go on to the subsequent step and fill in the essential details in these blank fields - DATE OF DEATH, Month, Day, Year, Telephone Number , Submitted by, SEXUALLY TRANSMITTED DISEASES STD, Primary lesion present Secondary, Neurosyphilis, Gonorrhea, UrethralCervical PID Other , Late latent year Late tertiary, Chlamydia, Fax , and Date Submitted.
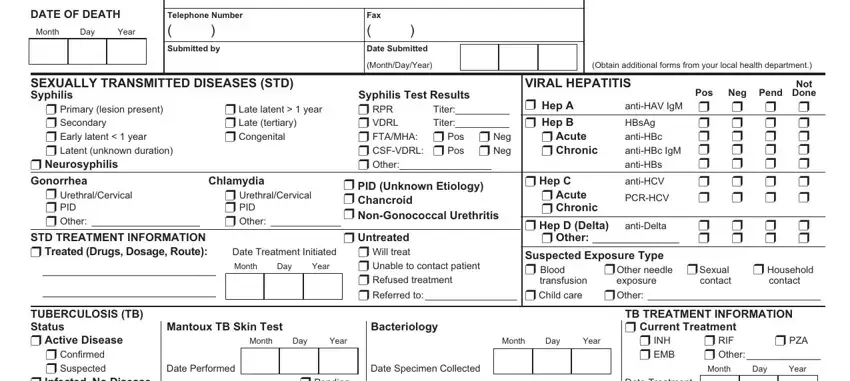
3. This step is normally straightforward - fill in every one of the empty fields in Infected No Disease, Pending, Convertor Reactor, Sites Pulmonary ExtraPulmonary , REMARKS, Results mm Not Done Source Smear, Chest XRay, Month, Day, Year, Date Performed, Normal Pending Not done , Other tests , Date Treatment, and Initiated to finish the current step.
Be extremely attentive while filling in Results mm Not Done Source Smear and Day, since this is the part where most people make some mistakes.
4. This next section requires some additional information. Ensure you complete all the necessary fields - Mumps, Paralytic Shellfish Poisoning, Pelvic Inflammatory Disease PID, FAX Pertussis Whooping Cough, Plague Human or Animal, LOCALLY REPORTABLE DISEASES If, This form is designed for health, and is a citable offense under, Failure to report is a citable, and PM revised page of - to proceed further in your process!
Step 3: Ensure that the information is correct and just click "Done" to proceed further. After getting afree trial account with us, you will be able to download California Form Pm110 or send it through email at once. The PDF form will also be available through your personal account page with all your adjustments. We don't share any information that you use whenever working with documents at our website.