The purpose of this document is to provide a review form for Cr 442 Certification. This form can be used by individuals who are seeking certification or by current certified professionals to self-evaluate their knowledge and skills in the area of Cr 442. The form covers five main topics: Concepts, Principles, Methods, Tools, and Applications. Within each topic, there are multiple subtopics that are covered. The goal of the review is to give the individual a broad understanding of all aspects related to Cr 442 so that they can confidently complete tasks within this area. This document is divided into two sections: Part 1 will provide an overview of the Cr 442 Certification process while Part 2 will be a review form specifically for individuals looking to become
| Question | Answer |
|---|---|
| Form Name | Cr 442 Certification Review Form |
| Form Length | 8 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 2 min |
| Other names | CR 442_Certificate _of_Awardabilit y_08 10_348552_7 ate of awardability form |
. . |
. . |
|
|
|
|
|
. . |
|
|
|
|
. . . . . |
. . |
|
|
. . |
||
|
. . . . . .. |
. |
. . . . . |
. . . . |
|
|
|
|
. . . . . . . . . |
|
||||||||
. . . .. .. . .. . |
. . |
.. |
|
. |
.. . . . . |
. . . . |
|
|
|
|
|
,..;:,...;.;... :..::.,. |
|
|
||||
. . . . |
. . : |
........ . :... . : ... |
. . . . |
|
|
|
|
|
.; |
|
||||||||
.. ... . .. ... .. . |
.. . . |
. |
:. |
. |
... . . |
|
|
RIGHTS :,~~~~ :.,::i~ij'~~,;:;':{::;;~~. . . |
;,;:,,,, |
|||||||||
. . . |
.. . .. |
.. |
.. .. .. |
.:. . . . |
|
:. ::;:."M~cH~GANDEPARTMENT. . .,,OF:. CIVIL |
. . |
|||||||||||
. . . . . .... |
..... .. . |
..: . .::. |
. . |
'.:. t .. ..C a d i l i a c place'::Suite |
.:3054 we&'Grand ~ ~ & &.Detroit,j |
~ i ~ h / ~ a ~ , @.:;i!'::.::~?.~::~0.. 2:,.._ ." |
, i:,.~.::;:. |
|||||||||||
. . . . . . . .. .. . ... ... .. . .. ... .. .. |
|
|
|
|
. . . . |
. , .. |
|
|||||||||||
|
.. .. .. |
. |
. . . |
. . |
. . . . . . .: : :,; |
.Office (313) |
~ (313)~ |
~ |
. :'.....: .>.'.::'. " . : . |
" |
. . . . . . |
|||||||
|
|
|
|
|
. . . . |
. . . |
||||||||||||
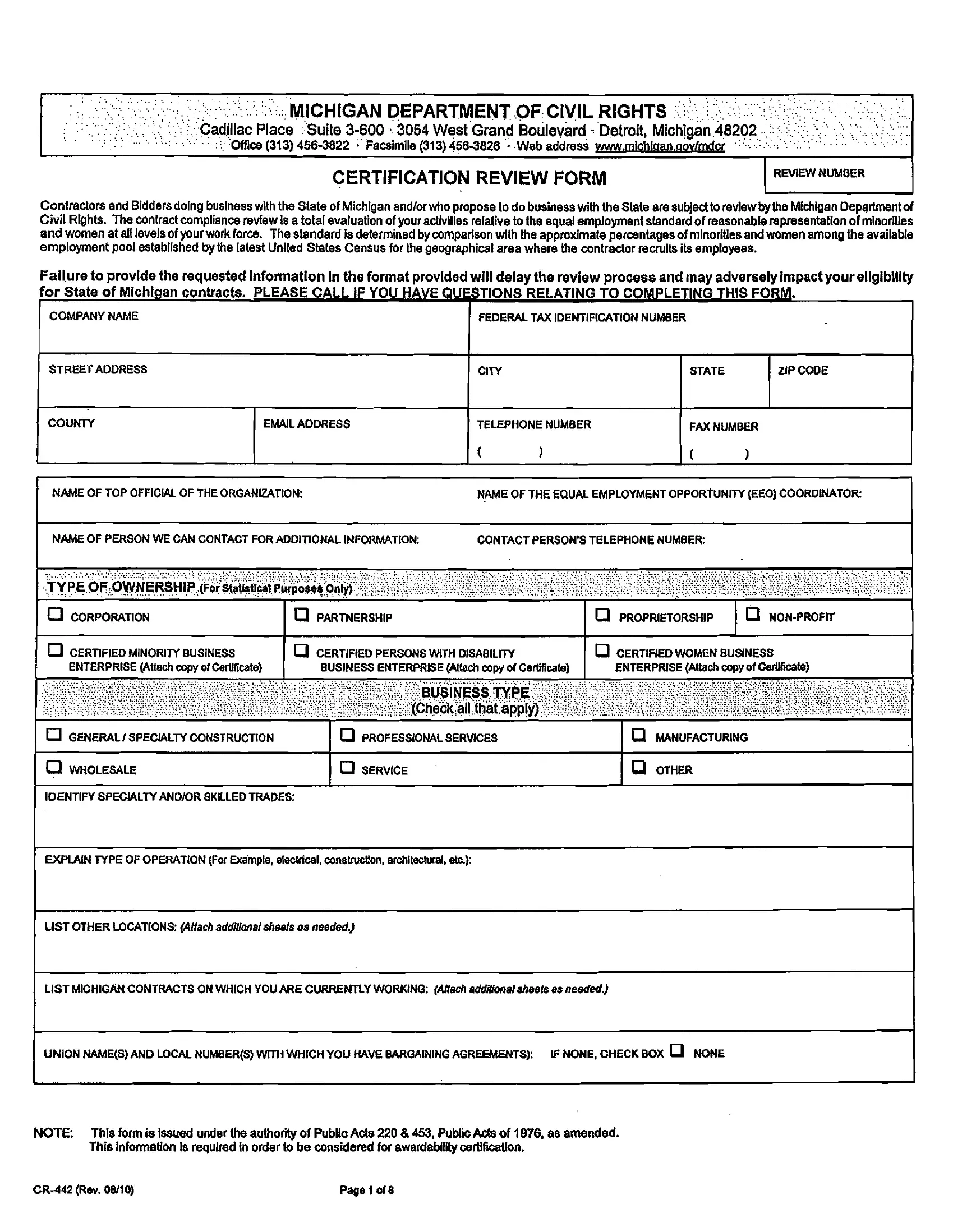
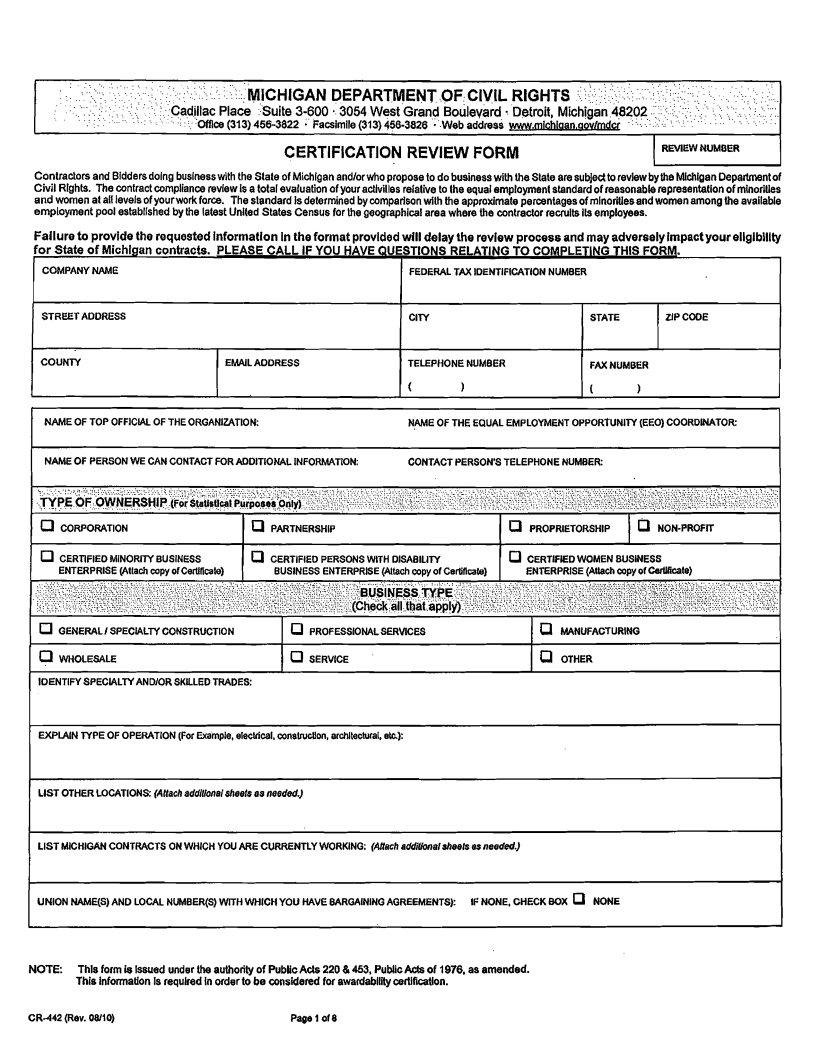
CERTIFICATION REVIEW FORM
REVIEW NUMBER
Contractors and Biddersdoing buslnesswlth the State of Michlganandlor who propose to do businesswith the State are subjedto reviewbythe Michi~anDepartmentof Civil Rights. The contractcompliance review is a total evaluation of your actlvilles relative to the equal employment standardof reasonablerepresentation of minorities and women at all levelsof yourwork force. The slandard is determined by comparisonwith the approximate percentagesof minoritiesandwomenamongthe available employment pool establishedby Ule latest United States Census for Ule geographicalarea where the contractor recruits ils employees.
Failure to provide the requestedInformation in the format providedwill delay the review processand may adverselyimpactyour ellgibllity
COMPANY NAME |
|
|
FEDERAL TAX IDENTIFICATIONNUMBER |
|
|
|
|||
STREET ADDRESS |
|
|
C I M |
|
|
STATE |
Z1P CODE |
|
|
COUNTY |
EMAILAODRESS |
TELEPHONE NUMBER |
|
FAX NUMBER |
|
||||
L |
|
- - - |
( |
1 |
|
( |
|
1 |
|
|
|
|
|
|
|
|
|
||
NAME OF TOP OFFICAL OF THE ORGANIZUION: |
N.ME OF THE EQUAL EMPLOYMENTOPPORTUNITY (EEO) COORDINATOR |
||||||||
NAME OF PERSONWE CAN CONTACT FORADDITIONAL INFORMATION: |
CONTACT PERSON'S TELEPHONE NUMBER |
|
|
|
|||||
TYPE OF OWNERSHIP or S ~ ~ U ~ ~UuCr ~p oI s iOnly)r |
,. |
. - |
|
|
|
, |
|
||
|
|
|
. |
. I |
|||||
0 CORPORATION |
|
a PARTNERSHIP |
|
|
0 PROPRIETORSHIP |
1 |
|||
CERTIFIEDMINORIM BUSINESS |
|
a CERTIFIED PERSONSWITH DISABILIM |
|
0 CERTIFIEDWOMEN BUSINESS |
|
||||
ENTERPRISE (Attach copy ofCertlficate1 |
BUSINESS ENTERPRISE (Attach CODYof CerlificaU |
ENTERPRISE(Attach COPYof CdliCate) |
|
||||||
GENERAL1SPECALNCONSTRUCTION |
0 PROFESSIONALSERVICES |
|
|
MANUFACTURING |
|
||||
0 WHOLESALE |
|
1 a SERVICE |
|
|
1 |
OTHER |
|
|
|
IOENTIFYSPEClALTYANDlOR SKILLEDTRADES:
EXPLAINM P E OF OPERATION(For Exa'mple, electrical, c o n s W o n , architectural, ek):
I LIST OTHER LOCATIONS: (Attachaddilfonaisneelsas needed)
LIST MICHIGANCONTRACTS ONWHICH YOU ARE CURRENTLYWORKING: (Attach addifionalaheels as needed)
- |
- |
- |
- |
--- |
- |
UNION NAME(S) AND LOCAL NUMBER(S) WITH WHICHYOU HAVEBARGAININGAGREEMENTS): |
IF NONE, CHECK BOX a NONE |
||||
-
I
I
NOTE: This form is Issued under the authority of PublicA& 220 & 453, PubllcA d s of 1976, as amended. This information is required in order to be considered for awadabllltycertification.
Page 1of 8 |
I COMPANY NAME |
|
I COUNTY |
IADDRESS (STREET) |
|
|
I a STATE EMPLOYMENTAGENCY (Provide Name) |
1 a UNIONS |
( 0 PRIVATEEMPLOYMENTAGENCIES |
0 WORD OF MOUTH |
a EQUAL OPPORTUNITYEMPLOYMENT |
|
USED INADS |
1 0
0
INTERNETa OTHER SOURCES
(Please Us1Below)
DO YOU USETARGETING RECRUITINGTECHNIQUESTO INCREASETHE NUMBER OF WOMEN, MINORITY GROUP PERSONS. AND PERSONSWIM DlSABlLmESWHO
APPLY FOR EMPLOYMENT? (Please specifically identityeach reccultmenltechnfque, 8.g.. name the newspapem Inwhich you will adveltlae, or the schoolsor organtzellonsyou will
|
contad) (Attach addifonalsheelsas needed.) |
|
|
ji? .;. ;:I(:; ; !::ii&;i;P:j- ;, .............,I,. .~::3<*,, ......;, |
|
|
|
|
|
|
|
|||||||||||
:.. :: |
:..:.... |
: |
::r. . |
. . .. . ... |
'..:l........i7.< |
;:; |
:.: |
;;.;,::,;................;<;::~;'~;;...,. .................,,;.j~~~;~~~ijj^$t~j+~ji ;~.;;.~7.;;.'.;;;:~:~:. ; ,. .l.' .,:i:.;.I:.:., |
. . . . . . |
|
....., :; ..,.: |
'..." |
.....................: |
;. |
|
|||||||
. |
A |
|
|
i,:;: :t.:l;i(>::............- |
.... |
? |
:::: |
< |
|
|||||||||||||
|
.......................... |
|
'" |
,:, ; > |
: |
|
.:...:: |
. |
|
i :;.i..i:<::.... |
y~ ~ |
|
|
|
|
|||||||
. ......... |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
.,,,:,,~:...................................: :; , ,:;,:~ ; :,; |
...::..::,. ....l..,i~..:..,..:i::,..:i~l:.:c:~~x:l~,:;.I:i:,:i:.ii.iI:y(~~~~.,I:~~I,.p .....................' |
~:~l:~:~;:~::~7..:1;:~.. .....,!.~:~. ........................~: ;~:;:~;:~:;:~;:~. ~ ~~~,.;~~:~77::;; |
~:..~~?~~~::~?:~~~::~::~;~. I...............: |
.:~,. |
||||||||||||||||||
|
. . . . . |
|
|
|
|
|||||||||||||||||
..... |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
[ |
|
WRITTENAPPLICATION |
(Send a copy of current ..application If not ~rovlded~revlouslv. |
|
1 |
0 RESUME |
1 D ORAL |
I |
D UNION I |
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I |
|
|
I |
|
I |
|
|
|
Teatlng Methods You Use: (Check allthat apply) - |
. - |
(I\
|
|
OTHER (OESCRIBE): |
|
|
|
|
I |
NAME: |
I TITLE: |
|
|
|
1 |
|
. , |
I |
|
. ., I |
|
. , . |
|
|
. . - |
. |
|||
|
. .. . . |
TRAINING PROGRAMS |
. . . . . . . . |
|
||
I |
|
|
|
|
I |
|
|
FORMALIINFORMAL: |
|
|
|
|
|
W W N :
I MANAGEMENT OR COLLEGETRAINEE PROGRAMSI HIGH SCHOOL
EXPLAIN:
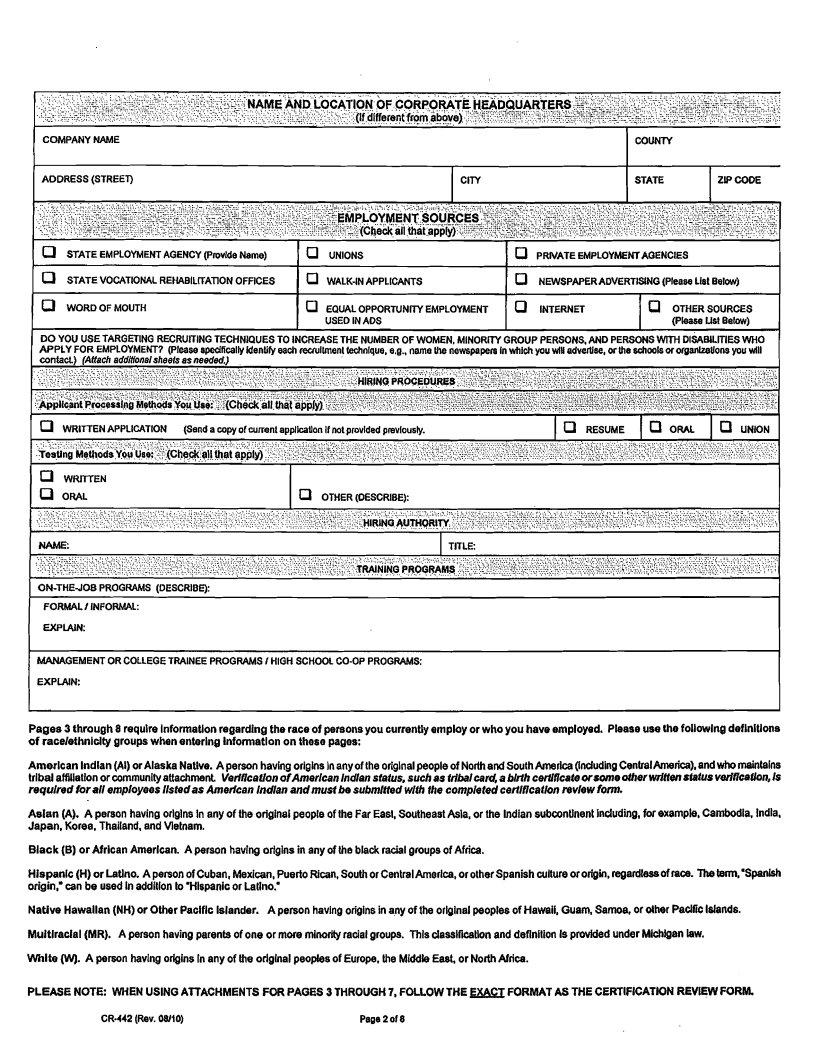
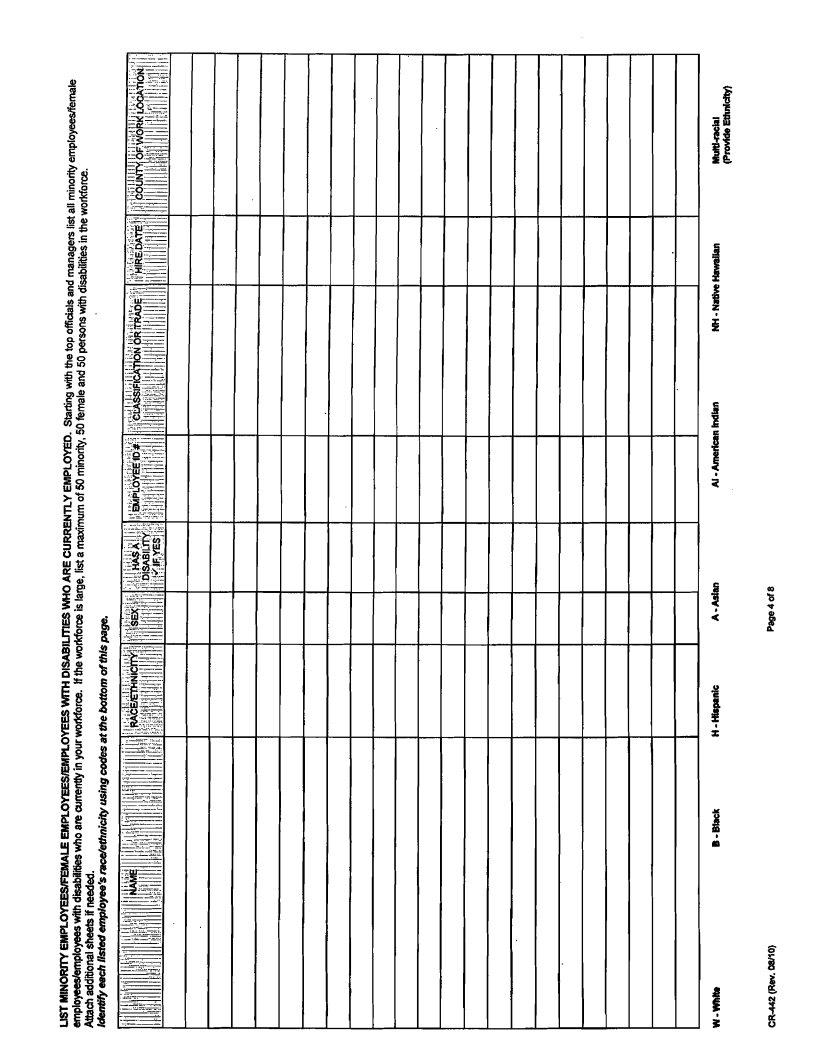
Pages 3 through 8 require lnformatlonregarding the raceof personsyou currenUy employ or who you haveemployed. Pleaseuse the following definltlons of racelethnlclty groups when enterlng lnformatlon on these pages:
Amerlcan lndlan (Al) or Alaska NaUve. A person having originsInany of the origlnalpeopleof NorthandSouthAmerica (Indudlng CenlralAmerica), andwho maintains trlbal affiliatfonor community attachment VedtlcatfonofAmerlcanlndlanstatus, such as tribalcard, a blrth cerlltlcateorsomedher writtensfatusverlflcallon, is requlredfor all employees llstedas Amedcan Indlan andmusf besubmlmdwlth fhe completedcertlflcatlon revlewfonn.
Asian (A). A person havlng orlgins h any of the orlginal peopleof the Far East, Southeast Asla, or the IndiansubconUnent Including, for example, Cambodia. Indla, Japan. Korea. Thailand, and Vietnam.
Black (B) or Afrlcan Amerlcan. A person havlng origins in any of Ule black racialgroups of Africa.
Hispanic (H) or Latlno. Aperson of Cuban, Mexican, PuertoRican, Southor CentralAmerica, or otherSpanishculture or origin, regardlessofrace. Thetem,'SpanM origin,' can be used Inaddition to 'Hispanic or Latino.'
Native Hawallan(NH) or Other Paclflc Islander. A person havlng origins in any of the origlnal peoples of Hawaii, Guam, Samoa, or dher PadficIslands.
Muitlraclal (MR). A person having parents of one or more minority racialgroups. This classifition and deflnitton Is provided under Michlgan law.
White 0.A person havlng orlgins Inany of Ule odglnal peoplesof Europe. Ule Middle East, or NorthAfrica.
PLEASE NOTE: WHEN USINGAllACHMENTS FOR PAGES 3 THROUGH 7, FOLLOWTHE FXAC'I: FORMAT AS THE CERTIFICATDN REVIEWFORM.
Page2 of 8 |
I |
I |
I |
I |
I |
I |
I |
|
|
s- |
|
|
~ |
O |
M |
~ |
||||||||
|
|
|
|
|
|
|
iI
m w
I
euoaredk w r
s u w e J o j
S3avu
=!ww
ruouadbwrar
e W w d
S 3 w
sa31)uardw
I
I
ruouad Wnor
su9-
S 3 w
lV3- 0 3 9 W O
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
~ O M s 3 l v S |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SN\113lNH331 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SlVNOlSS%OYd |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SU39NWY '8 m 9 1 u o |
elem9 |
b o r r l ~ t |
saakldur3 |
a N |
H N |
I V |
V |
H |
El |
M |
Y R |
H N |
I V |
V |
H |
B |
M |
W L |
|
|
|
|
|
|
|
|
|
|
||||||
lopol |
lopol |
|
|
|
|
|
|
|
|
|
|
|
|
|
S3RI09UV3 |
aor
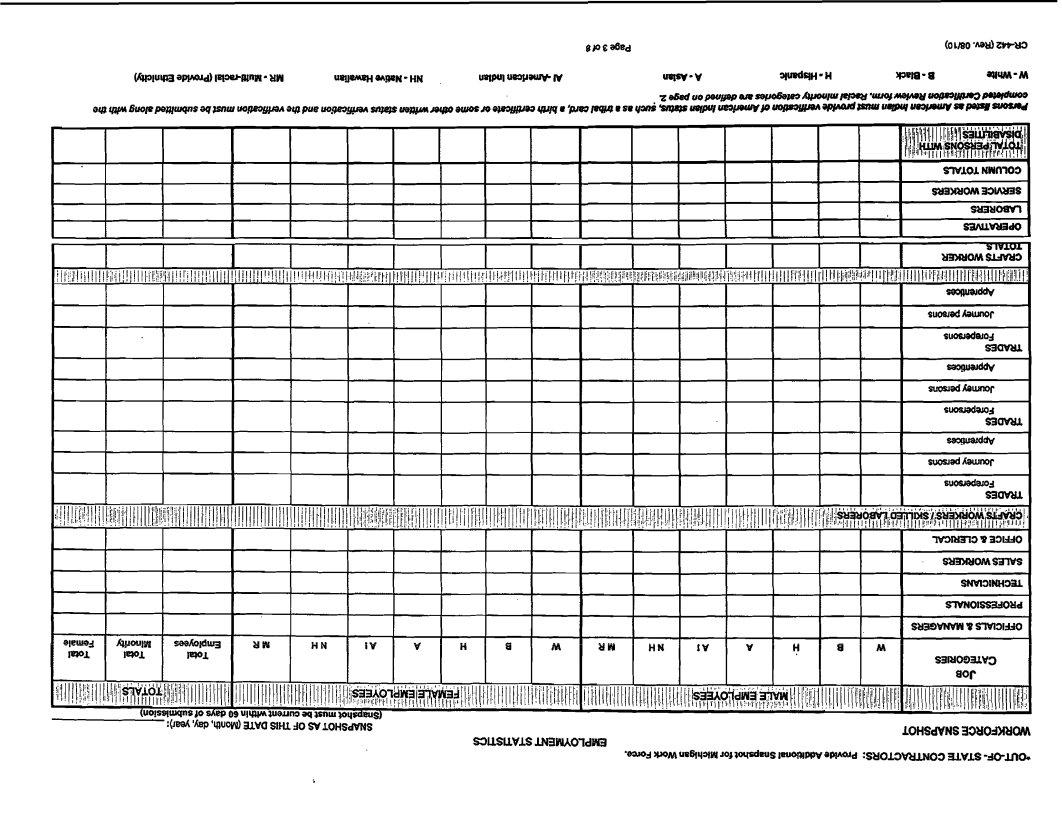
( u o l s s ( dap~ ~ 09~ U l W W W m acl muwqsdsus)
:(J& 'h'wuoyy) uva sliu 40 SV LOHSWNS |
IOHSdVNS33MOdNiQh4 |
|
S=)USUVlSIMMO'ldtEl
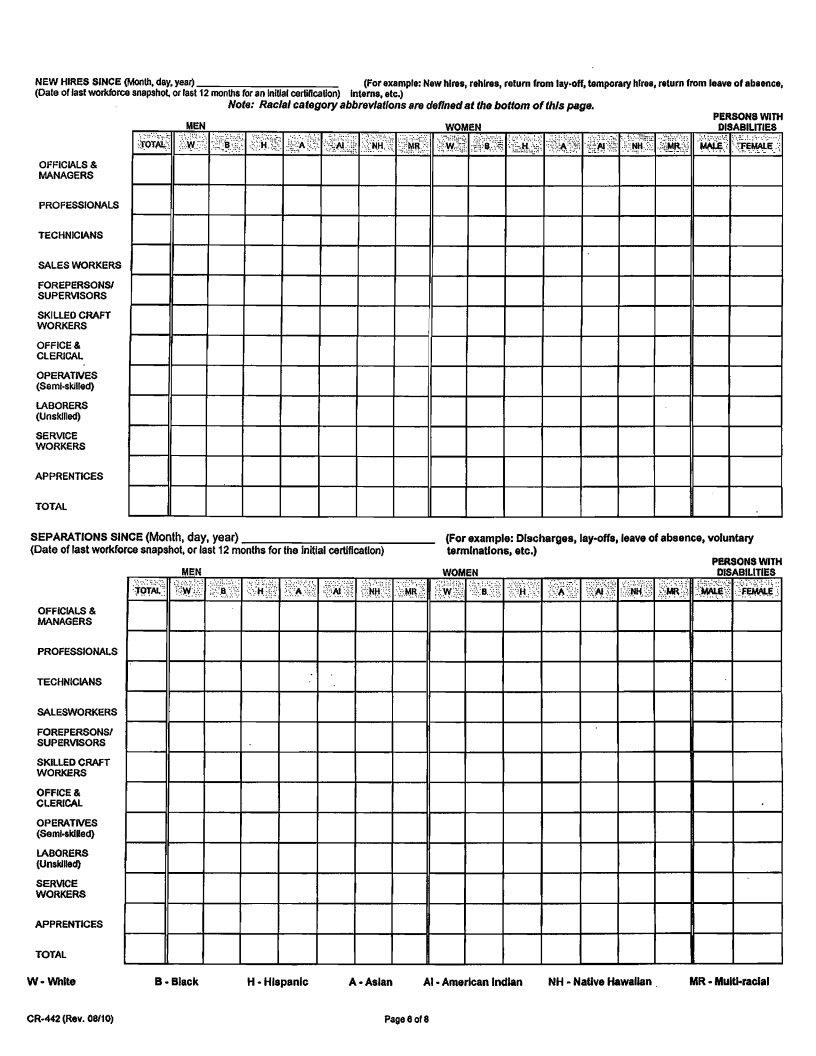
NEW HIRES SINCE (Month, day. year) (Date of last woikforcesnapshot. or last
(For example: New hlres, rehlres, return from
Note: Raclalcategoryabbrevlatlonsere deflnedat the bottom of thls page.
PERSONSWITH
OFFlClALS &
MANAGERS
PROFESSIONALS
TECHNICIANS
SALES WORKERS
FOREPERSONSI
SUPERVISORS
SKILLED CRAFT
WORKERS
OFFICE &
CLERICAL
OPERATNES
LABORERS (Unskilled)
SERVICE
WORKERS
APPRENTICES
TOTAL
SEPARATIONS SINCE (Month, day, year)
(Date of last workforcesnapshot, or last 12 monthsfor the initial certiflcatlon)
OFFICIALS &
MANAGERS
PROFESSIONALS
TECHNICIANS
SALESWORKERS
FOREPERSONS/
SUPERVISORS
SKILLED CRAFT
WORKERS
OFFICE &
CLERICAL
OPERATIVES (SemCskllled)
LABORERS (Unskilled)
SERVICE
WORKERS
APPRENTICES
TOTAL
W - Whlte |
B - Black |
- |
A |
H - Hlspanlc |
(For example: Discharges,
PERSONSWITH
Al |
NH - Natlve Hawalian |
MR |
Page 8 of 8 |
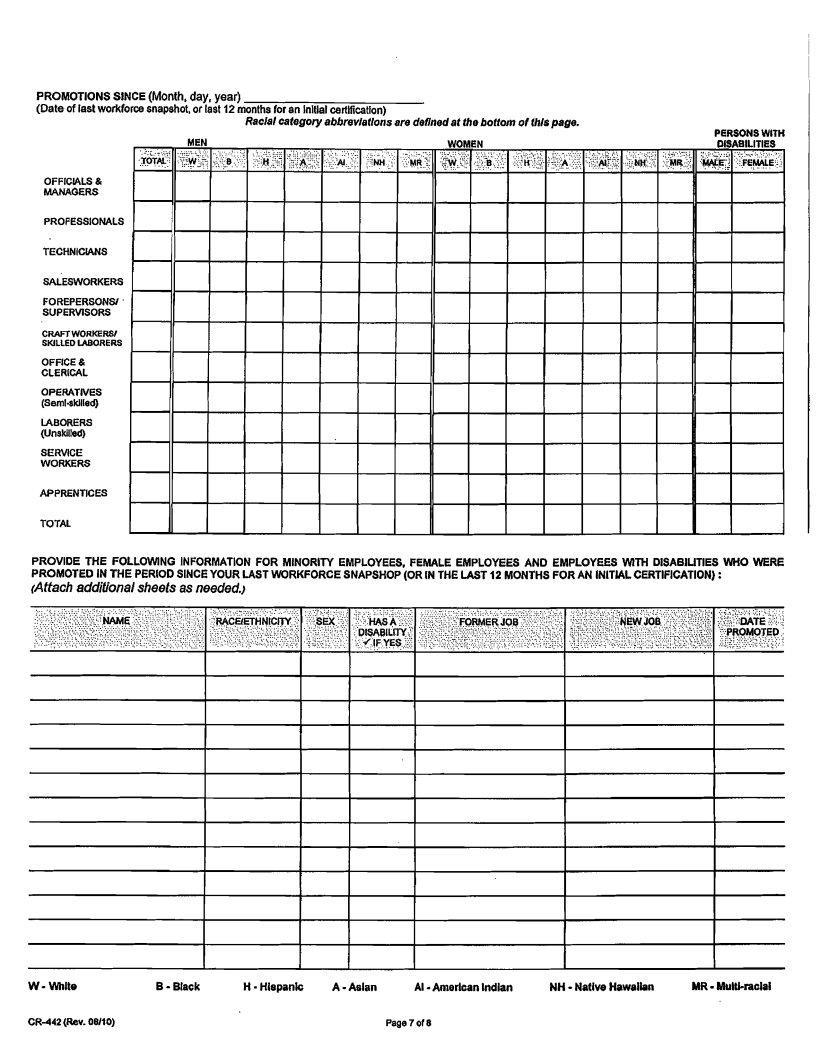
PROVIDE THE FOLLOWING INFORMATION FOR MINORITY EMPLOYEES, FEMALE EMPLOYEES AND EMPLOYEES WITH DISABILITIES WHO WERE PROMOTED IN THE PER100 SINCE YOUR LAST WORKFORCE SNAPSHOP (OR IN THE LAST 12 MONTHS FOR AN INlTlAL CERTIFICATION) :
(Attach additional sheets as needed.)
W - Whlte |
B - Black |
H - Hlepanlc |
A |
Al |
NH |
MR |
CR442 (Rev. OUIO) |
Page 7 of 8 |
I . |
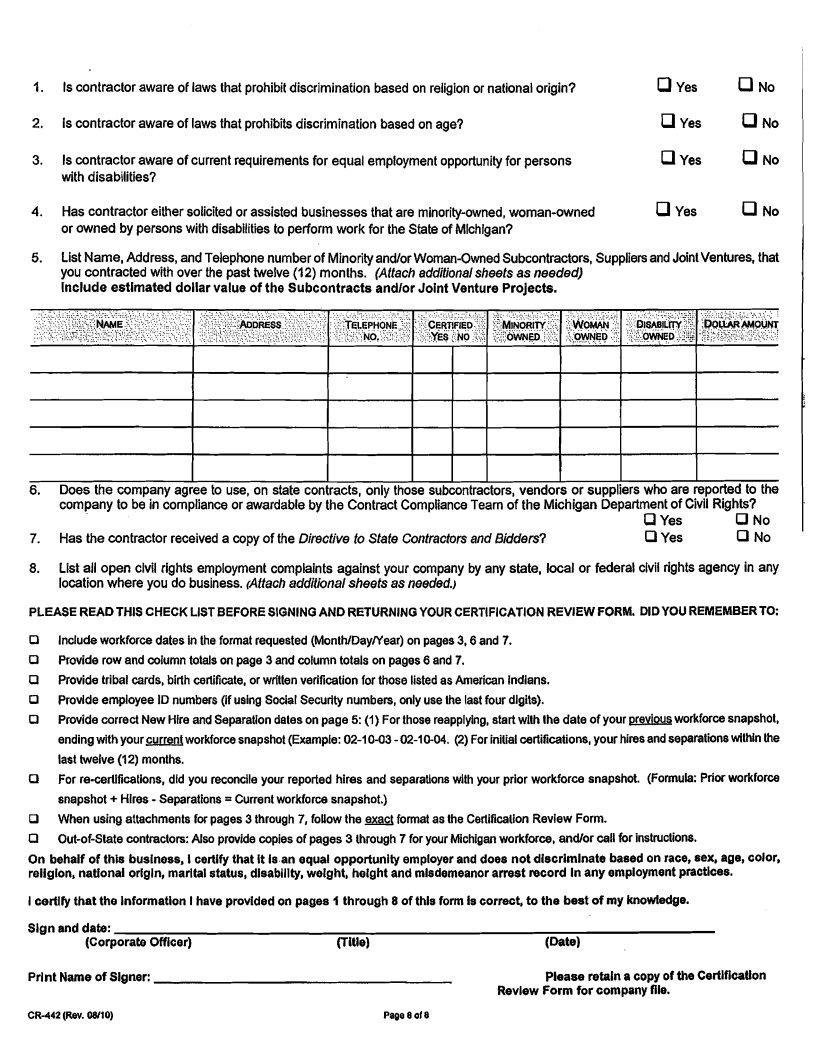
Is contractor aware of laws that prohibit discrimination based on religion or national origin? |
0yes |
0No |
2. |
Is contractor aware of laws that prohibits discrimination based on age? |
a yes |
0No |
3. |
Is contractor aware of current requirements for equal employment opportunity for persons |
yes |
0No |
|
with disabilities? |
|
|
4. |
Has contractor either solicited or assisted businesses that are |
a Yes |
0No |
|
or owned by persons with disabilities to perform work for the State of Michigan? |
|
|
5. |
List Name, Address, and Telephone number of Minorityand/or |
||
|
you contracted with over the past twelve (12) months. (Aftach additional sheets as needed) |
|
|
Include estimated dollar value of the Subcontracts andlor Joint Venture Projects.
~. . |
||||||||||||||||||||||||||
.................... . . . . . . . |
" |
. . . |
. . . . |
. . . |
. . . . . . . . |
. . . . . . . . . . . . . . . . . .' |
. . .:..:. |
. . . . . . . |
: . : |
. . . . . . |
. |
. |
|
|
|
::L,(,., I |
..............: |
>: : : . |
.: :.... |
'..?... |
:.,, |
|
::. |
...........::..:...::.>....". : |
||
............................................ |
|
;;s+&.;;j |
|
|
|
...; |
. . . |
. |
. . . . |
. . . . . . . . |
. . |
, |
';.'...%.;..:.....; |
<i$;&g&"Gb |
||||||||||||
|
|
|
" |
............. |
|
|
|
|
|
|
|
|
................................... |
|
..'..F. |
|
|
|||||||||
,:.;/:<:.:; |
.... |
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
;!,N<i |
!;,:;B. ,&,. . . . . . . ..CMF. . ..$. . . . |
|||||||||||||||||||||||
.............................................. |
|
|
. . |
": :.cl....(:::,.::: |
|
,..;; |
|
|
|
|
|
|
|
- |
|
|
|
|
;. |
|
|
|||||
; |
::.( |
. . . . |
|
|
|
|
|
|
|
|
. . . . . . . . . . ..if<.ew,=~,. , .: |
......... |
: :. |
|
|
|||||||||||
........ |
|
::;;,j,:,I:;+~:..:yj~ |
:,,:.: |
|
|
|
|
|
:;..:;.::;.&s |
j?X;I ;.. |
|
|
|
|
|
|
|
|
||||||||
. . . .. . . . . . . . |
. .,. |
. . . . . . . . .... |
,:;:..;: |
............... |
|
|
..::.. |
|
|
. . . . . . . . .;:::;;; |
:;OWED |
.:; |
:8 + : ~ ~ . : o |
|||||||||||||
|
|
................................................ |
|
|
|
|
|
|
r |
: : ' I |
|
|
|
|
||||||||||||
6 . |
Does the company agree to use, on state contracts, only those subcontractors, vendors or suppliers who are reported to the |
||
|
company to be in compliance or awardable by the Contract Compliance Team of the Michigan Department of Civil Rights? |
||
|
|
r;ll Yes |
No |
7. |
Has the contractor received a copy of the Directive fo Stafe Contractors and Bidders? |
0 Yes |
a No |
8.List all open clvil rights employment complaints against your company by any state, local or federal clvil rights agency in any locationwhere you do business. (Aftach additional sheets as needed.)
PLEASE READTHIS CHECK LIST BEFORE SIGNINGAND RETURNINGYOUR CERTIFICATION REVIEW FORM. DIDYOU REMEMBERTO:
0Includeworkforce dates in the format requested (Monlh/DaylYear) on pages 3,6 and 7.
0Provide row and column totals ON page 3 and column totals on pages 6 and 7.
O Provide tribal cards, birth certificate, or wrilten verification for those listed as American Indians. Provlde employee ID numbers (if using Social Security numbers, only use the last four dlgits).
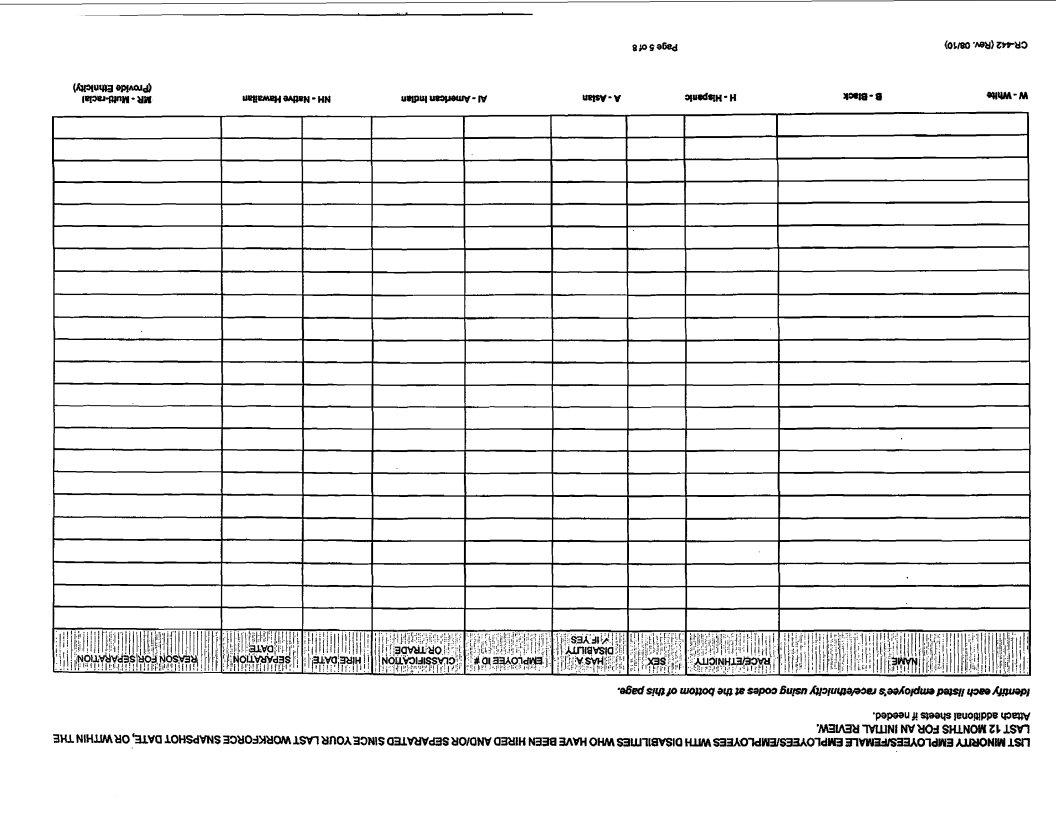
0Provide correct New Hire and Separationdales on page 5: (I)For those reapplying, start wllh the date of your previousworkforce snapshol,
endingwithyour current workforce snapshot (Example:
0For
R When using attachments for pages 3 through 7, follow the EXACT format as the Certification Review Form.
R
On behalf of this business, Icertify that it Is an equal opportunity employer and does not discriminate based on race, sex, age, color, reiiglon, natlonai origln, marltal status, dlsablllty, weight, height and misdemeanor arrest record Inany employment ptactlces.
Icertlfy that the Information Ihave provlded on pages 4 through 8 of this form is correct, to the best of my knowledge.
Slgn and date: |
|
|
(Corporate Officer) |
(Title) |
(Date) |
Prlnt Name of Signer: |
|
Please retain a copy of the CertlflcaUon |
|
|
Revlew Form for company file. |
CR442 (Rev. 06/10) |
Page 8 of 8 |