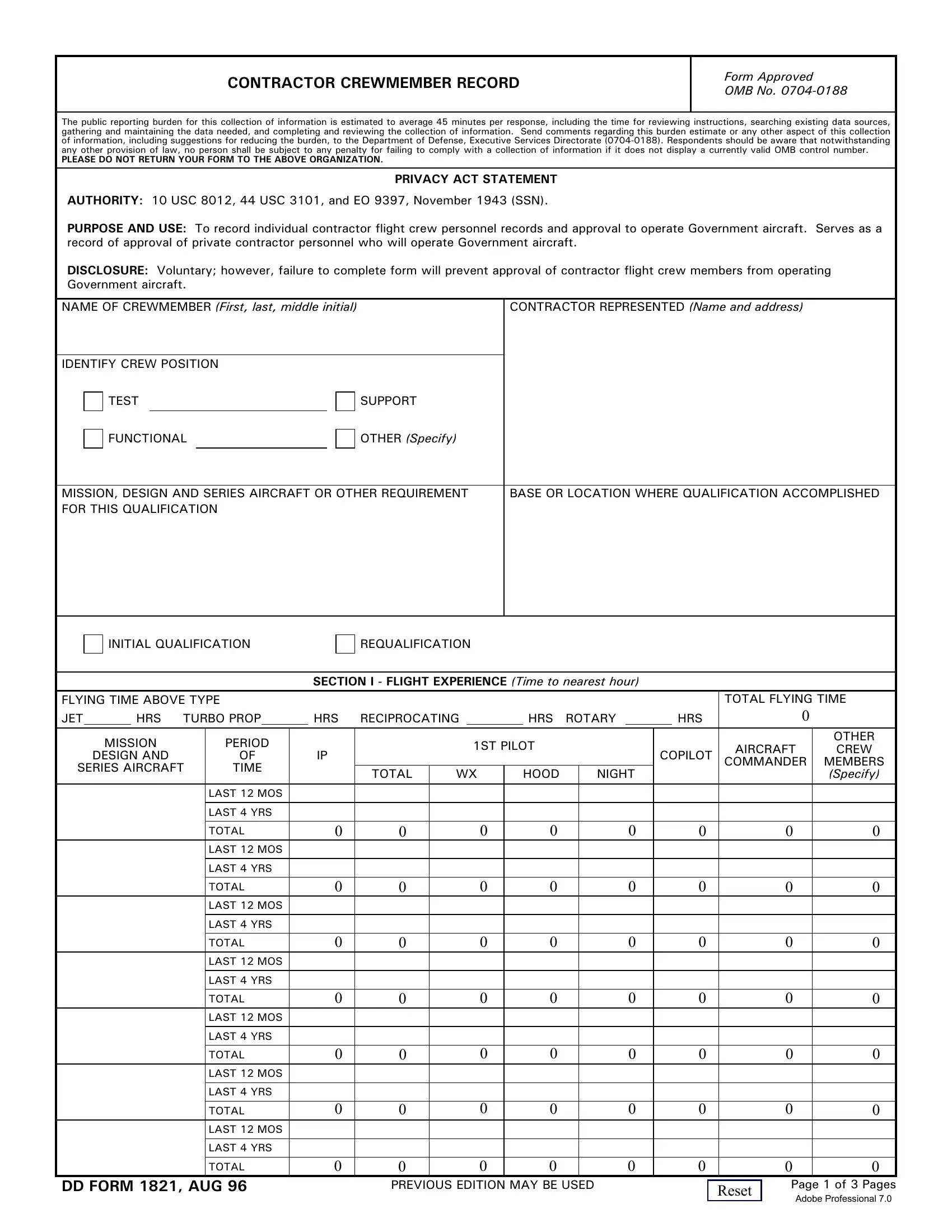
Dd1821 form is used to document an individual's admission, treatment and/or discharge from a psychiatric hospital or other mental health facility. The form consists of information such as the patient's name, date of birth, and current address, as well as admissions and discharges dates, diagnoses, medications administered, and other relevant information. The dd1821 form is an important tool for tracking an individual's care and progress. If you are looking to order dd1821 forms for your hospital or mental health facility, you can visit our website to learn more about our products and services. We offer a variety of dd1821 forms that are designed to meet your specific needs. Our team can also help you customize the forms to ensure
| Question | Answer |
|---|---|
| Form Name | Dd1821 Form |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | dd 1821 fillable, dd1821 form, dd form 1821 pdf, dd form 1821 |
CONTRACTOR CREWMEMBER RECORD
Form Approved OMB No.
The public reporting burden for this collection of information is estimated to average 45 minutes per response, including the time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information. Send comments regarding this burden estimate or any other aspect of this collection of information, including suggestions for reducing the burden, to the Department of Defense, Executive Services Directorate
PLEASE DO NOT RETURN YOUR FORM TO THE ABOVE ORGANIZATION.
PRIVACY ACT STATEMENT
AUTHORITY: 10 USC 8012, 44 USC 3101, and EO 9397, November 1943 (SSN).
PURPOSE AND USE: To record individual contractor flight crew personnel records and approval to operate Government aircraft. Serves as a record of approval of private contractor personnel who will operate Government aircraft.
DISCLOSURE: Voluntary; however, failure to complete form will prevent approval of contractor flight crew members from operating Government aircraft.
NAME OF CREWMEMBER (First, last, middle initial) |
|
CONTRACTOR REPRESENTED (Name and address) |
|||
|
|
|
|||
IDENTIFY CREW POSITION |
|
|
|||
TEST |
SUPPORT |
|
|||
|
|
|
|
|
|
FUNCTIONAL |
OTHER (Specify) |
|
|||
|
|
|
|
||
|
|
||||
MISSION, DESIGN AND SERIES AIRCRAFT OR OTHER REQUIREMENT |
BASE OR LOCATION WHERE QUALIFICATION ACCOMPLISHED |
||||
FOR THIS QUALIFICATION |
|
|
|||
|
|
|
|
|
|
INITIAL QUALIFICATION
REQUALIFICATION
SECTION I - FLIGHT EXPERIENCE (Time to nearest hour)
FLYING TIME ABOVE TYPE |
|
|
|
|
|
|
|
|
|
|
TOTAL FLYING TIME |
|||||
JET |
|
HRS TURBO PROP |
HRS |
RECIPROCATING |
|
HRS |
ROTARY |
|
HRS |
0 |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MISSION |
PERIOD |
|
|
|
1ST PILOT |
|
|
|
|
AIRCRAFT |
OTHER |
||||
|
IP |
|
|
|
|
COPILOT |
CREW |
|||||||||
|
DESIGN AND |
OF |
|
|
|
|
|
|
|
COMMANDER |
MEMBERS |
|||||
SERIES AIRCRAFT |
TIME |
|
TOTAL |
WX |
|
HOOD |
NIGHT |
|
|
|
(Specify) |
|||||
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LAST 12 MOS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LAST 4 YRS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
TOTAL |
0 |
0 |
|
|
0 |
0 |
0 |
0 |
0 |
0 |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LAST 12 MOS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LAST 4 YRS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
TOTAL |
0 |
0 |
|
|
0 |
0 |
0 |
0 |
0 |
0 |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LAST 12 MOS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LAST 4 YRS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
TOTAL |
0 |
0 |
|
|
0 |
0 |
0 |
0 |
0 |
0 |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LAST 12 MOS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LAST 4 YRS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
TOTAL |
0 |
0 |
|
|
0 |
0 |
0 |
0 |
0 |
0 |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LAST 12 MOS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LAST 4 YRS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
TOTAL |
0 |
0 |
|
|
0 |
0 |
0 |
0 |
0 |
0 |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LAST 12 MOS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LAST 4 YRS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
TOTAL |
0 |
0 |
|
|
0 |
0 |
0 |
0 |
0 |
0 |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LAST 12 MOS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LAST 4 YRS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
TOTAL |
0 |
0 |
|
|
0 |
0 |
0 |
0 |
0 |
0 |
|||
DD FORM 1821, AUG 96 |
PREVIOUS EDITION MAY BE USED |
|
Page 1 of 3 Pages |
|
Reset |
||||
|
|
Adobe Professional 7.0 |
||
|
|
|
SECTION II - FLIGHT CHECK (Instructor fill in remarks where applicable)
1. PREFLIGHT INSPECTION |
|
|
|
7. |
|
|
|
AND FORMS |
|
|
|
|
PROCEDURES |
|
|
|
|
|
|
|
|
|
|
2. EMERGENCY ESCAPE |
|
|
|
8. PRELANDING CHECK, TRAFFIC |
|
|
|
PROCEDURES |
|
|
|
|
PATTERN AND LANDINGS |
|
|
|
|
|
|
|
|
|
|
3. PRESTART COCKPIT PRO- |
|
|
|
9. |
POSTFLIGHT INSPECTION |
|
|
CEDURE AND ENGINE START |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. COMMUNICATIONS AND |
|
|
|
10. ACCOMPLISHMENT OF FORMS |
|
|
|
TAXI PROCEDURES |
|
|
|
|
AND AIRCRAFT SECURITY |
|
|
|
|
|
|
|
|
|
|
5. PRETAKEOFF COCKPIT CHECK |
|
|
|
11. INSTRUMENT PROFICIENCY |
|
|
|
AND ENGINE RUNUP |
|
|
|
|
CHECK |
|
|
|
|
|
|
|
|
|
|
6. TAKEOFF AND FLIGHT |
|
|
|
12. OTHER (Specify) |
|
|
|
PROCEDURES |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
SECTION III - ADDITIONAL REQUIREMENTS (Fill in where applicable) |
|
||||
REQUIREMENT |
CHECKED BY |
GRADE |
DATE AND PLACE |
HOURS |
|||
|
|
|
|
|
|
|
|
13. PHYSICAL EXAMINATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
14. PHYSIOLOGICAL/ATTITUDE |
|
|
|
|
|
|
|
INDOCTRINATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
15. PRESSURE SUIT TRAINING |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
16. GROUND SCHOOL (By Subject) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
AIRCRAFT GENERAL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
AIRCRAFT PREFLIGHT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
AIRCRAFT EMERGENCY PROCEDURE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ENGINE SYSTEM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OXYGEN SYSTEM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
AIR CONDITIONING |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PRESSURIZATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FUEL SYSTEM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
INSTRUMENT SYSTEM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ELECTRICAL SYSTEM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
HYDRAULIC POWER SYSTEM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
UTILITY SYSTEM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FLIGHT CONTROL SYSTEM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
AUTO PILOT SYSTEM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ENGINE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
COMMUNICATIONS & NAVIGATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ROTARY SYSTEM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OTHER REQUIREMENTS AS STATED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
IN APPROVED CONTR OPR PROCD |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
17. QUESTIONNAIRE ON AIRCRAFT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
18. FLIGHT SIMULATOR |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
19. SURVIVAL SCHOOL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
20. OTHER (Specify) |
|
|
|
|
|
|
|
21. HAVE YOU EVER HAD AN AIRCRAFT ACCIDENT (as defined by FAR or military procedures) OR PHYSIOLOGICAL REACTION (e.g., hypoxia, decompression sickness, hyperventilation, spatial disorientation) AS A PILOT, OR OTHER CREW MEMBER? (If yes, explain.)
22. HAVE YOU EVER BEEN CHARGED WITH A FLYING VIOLATION? (If so, state the violation and circumstances.)
23. REMARKS (For additional space use blank sheet.)
DD FORM 1821, AUG 96
Reset
Page 2 of 3 Pages
CERTIFICATION OF QUALIFICATION
This is to certify that
(Name and Crew Position)
has satisfactorily completed the training or special qualification indicated hereon:
YEAR |
TRAINING OR SPECIAL QUALIFICATIONS |
DATE |
CERTIFYING |
|
COMPLETED |
OFFICIAL |
|||
|
|
|||
|
|
|
|
|
|
GROUND PHASE |
|
|
|
|
|
|
|
|
|
WRITTEN EXAMINATION |
|
|
|
|
|
|
|
|
|
EMERGENCY PROCEDURES |
|
|
|
|
|
|
|
|
|
CONTRACTOR FLIGHT OPERATIONS PROCEDURES |
|
|
|
|
|
|
|
|
|
EGRESS TRAINING |
|
|
|
|
|
|
|
|
|
PHYSIOLOGICAL TRAINING |
|
|
|
|
|
|
|
|
|
OTHER (Specify)1 |
|
|
|
|
|
|
|
|
|
FLIGHT PHASE |
|
|
|
|
|
|
|
|
|
PROFICIENCY |
|
|
|
|
|
|
|
|
|
INSTRUMENT |
|
|
|
|
|
|
|
|
|
OTHER (Specify)1 |
|
|
|
|
|
|
|
|
|
GROUND PHASE |
|
|
|
|
|
|
|
|
|
WRITTEN EXAMINATION |
|
|
|
|
|
|
|
|
|
EMERGENCY PROCEDURES |
|
|
|
|
|
|
|
|
|
CONTRACTOR FLIGHT OPERATIONS PROCEDURES |
|
|
|
|
|
|
|
|
|
EGRESS TRAINING |
|
|
|
|
|
|
|
|
|
PHYSIOLOGICAL TRAINING |
|
|
|
|
|
|
|
|
|
OTHER (Specify)1 |
|
|
|
|
|
|
|
|
|
FLIGHT PHASE |
|
|
|
|
|
|
|
|
|
PROFICIENCY |
|
|
|
|
|
|
|
|
|
INSTRUMENT |
|
|
|
|
|
|
|
|
|
OTHER (Specify)1 |
|
|
|
|
|
|
|
1 Formation, Refueling, Night or other special maneuver requirements.
SECTION IV - CERTIFICATIONS
I certify that I have read and understand all pertinent technical orders, handbooks, contractor's operating procedures, and pilot's operating instructions pertaining to the above aircraft.
DATE
SIGNATURE OF CREWMEMBER
The above named crewmember has/has not demonstrated proficiency in, and has/has not a satisfactory knowledge of
MDS aircraft and has/has not satisfactorily completed the flight requirements for the type of flight check indicated above, and is/is not fully qualified in this type aircraft.
The checkout consisted of |
|
hours dual, |
|
hours solo, |
|
landings from right (or rear) seat, |
|||
and |
|
landings from left (or front) seat. |
|
|
|
|
|||
|
|
|
|
|
|||||
DATE |
|
BASE OR HOME STATION OF INSTRUCTOR |
|
TYPED OR PRINTED NAME OF INSTRUCTOR |
|||||
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
SIGNATURE OF INSTRUCTOR |
||
DD FORM 1821, AUG 96 |
|
Page 3 of 3 Pages |
|
Reset |
|||
|
|
||
|
|
|