
Informacin can be filled out online easily. Simply make use of FormsPal PDF editor to do the job in a timely fashion. Our tool is continually developing to deliver the very best user experience possible, and that is thanks to our resolve for continuous enhancement and listening closely to customer comments. Here is what you would have to do to get started:
Step 1: Hit the "Get Form" button at the top of this page to get into our tool.
Step 2: This tool gives you the opportunity to modify most PDF forms in a variety of ways. Transform it by writing your own text, adjust what is already in the document, and add a signature - all at your fingertips!
It's an easy task to complete the form with this detailed guide! This is what you need to do:
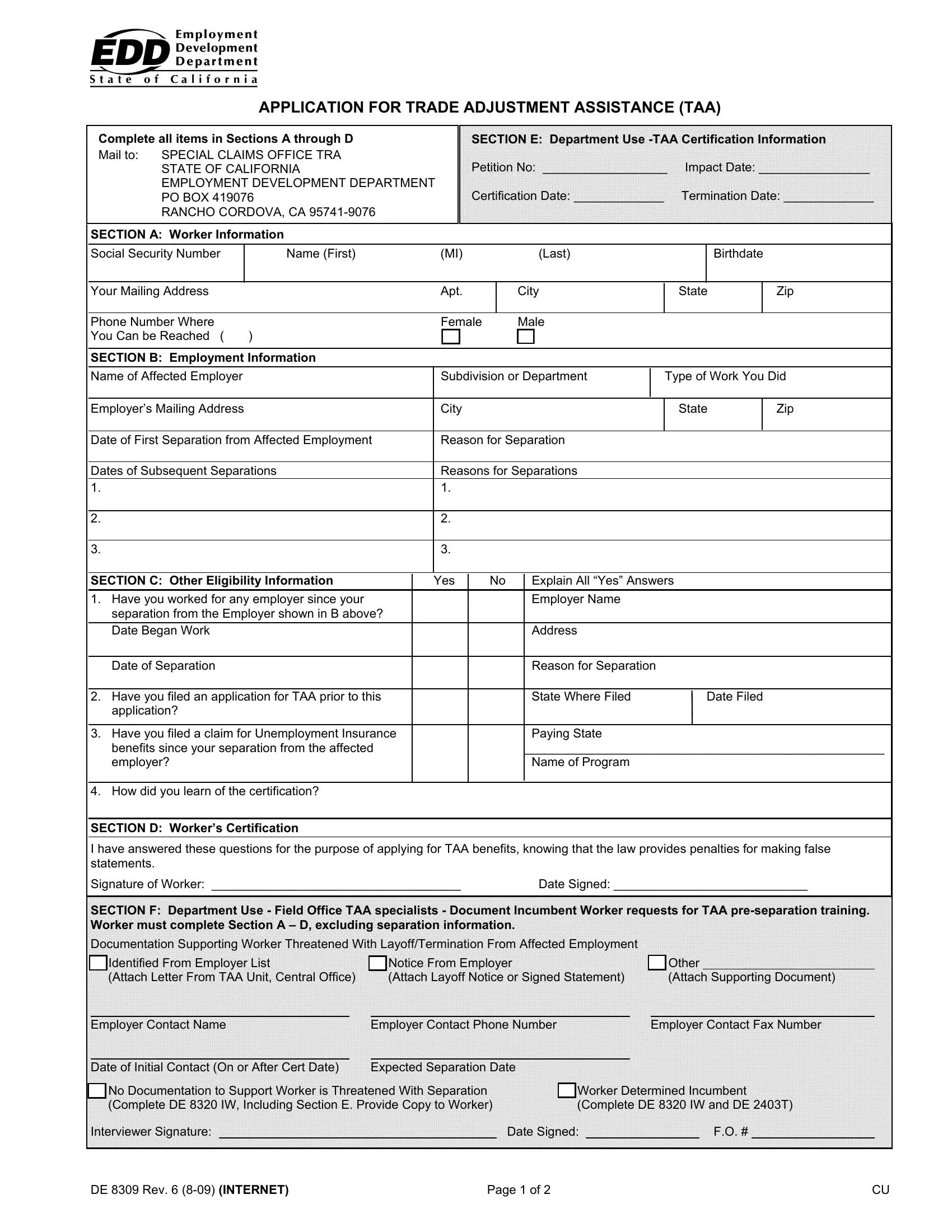
1. It's very important to complete the Informacin properly, therefore be attentive while filling out the sections including these specific blank fields:
2. Once this array of fields is finished, it is time to put in the essential details in Date of Separation Have you filed, application, Have you filed a claim for, benefits since your separation, How did you learn of the, SECTION D Workers Certification, I have answered these questions, Signature of Worker, Date Signed, SECTION F Department Use Field, Documentation Supporting Worker, Identified From Employer List, Notice From Employer Attach Layoff, Other Attach Supporting Document, and Employer Contact Name so you can proceed further.
People who use this form frequently make mistakes while filling out benefits since your separation in this section. Be sure to re-examine whatever you enter right here.
Step 3: Ensure the details are correct and then click on "Done" to finish the project. Sign up with FormsPal right now and immediately get Informacin, all set for download. Every edit you make is handily preserved , making it possible to edit the file later on anytime. We don't share or sell any details that you use when dealing with documents at our website.