The Department of Homeland Security (DHS) is one of the most important agencies in the United States government. Its responsibilities range from counterterrorism to protecting our nation's borders. As a result, it's important that you know how to apply for DHS jobs if you're interested in working for this agency. In this blog post, we'll walk you through the process of filling out the DHS 18A form. We'll also provide some tips on how to make your application stand out from the rest. So if you're ready to start your career with DHS, keep reading!
| Question | Answer |
|---|---|
| Form Name | Dhs 18A Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | DHS 0018 A_162674_7 dhs michigan hearing request withdrawal what is ah register # form |
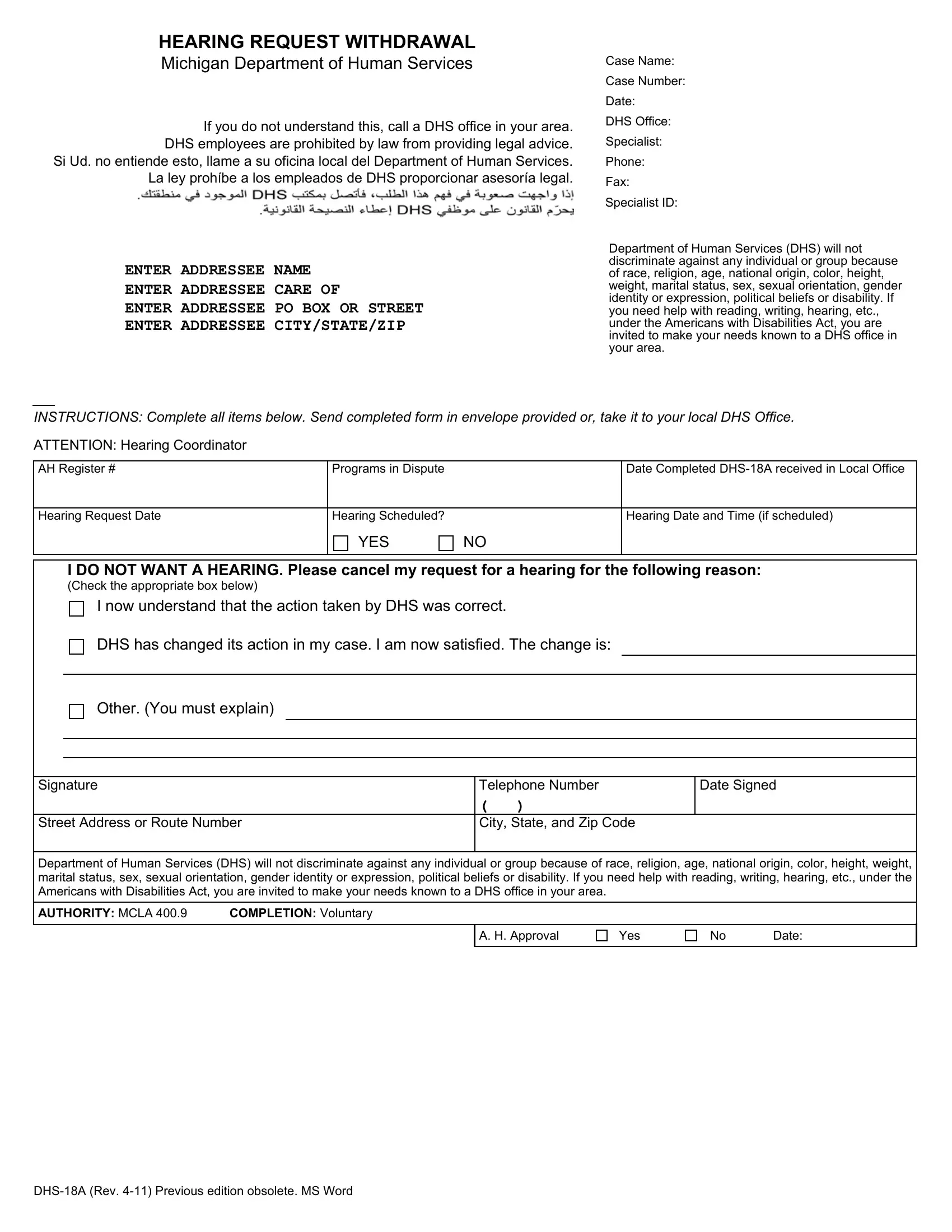
HEARING REQUEST WITHDRAWAL
Michigan Department of Human Services
Case Name:
If you do not understand this, call a DHS office in your area. DHS employees are prohibited by law from providing legal advice.
Si Ud. no entiende esto, llame a su oficina local del Department of Human Services. La ley prohíbe a los empleados de DHS proporcionar asesoría legal.
ENTER ADDRESSEE NAME
ENTER ADDRESSEE CARE OF
ENTER ADDRESSEE PO BOX OR STREET
ENTER ADDRESSEE CITY/STATE/ZIP
Case Number:
Date:
DHS Office:
Specialist:
Phone:
Fax:
Specialist ID:
Department of Human Services (DHS) will not discriminate against any individual or group because of race, religion, age, national origin, color, height, weight, marital status, sex, sexual orientation, gender identity or expression, political beliefs or disability. If you need help with reading, writing, hearing, etc., under the Americans with Disabilities Act, you are invited to make your needs known to a DHS office in your area.
INSTRUCTIONS: Complete all items below. Send completed form in envelope provided or, take it to your local DHS Office.
ATTENTION: Hearing Coordinator
AH Register # |
Programs in Dispute |
|
Date Completed |
|
|
|
|
Hearing Request Date |
Hearing Scheduled? |
|
Hearing Date and Time (if scheduled) |
|
YES |
NO |
|
|
|
|
|
I DO NOT WANT A HEARING. Please cancel my request for a hearing for the following reason:
(Check the appropriate box below)
I now understand that the action taken by DHS was correct.
DHS has changed its action in my case. I am now satisfied. The change is:
Other. (You must explain)
Signature |
Telephone Number |
Date Signed |
|
( |
) |
Street Address or Route Number |
City, State, and Zip Code |
|
Department of Human Services (DHS) will not discriminate against any individual or group because of race, religion, age, national origin, color, height, weight, marital status, sex, sexual orientation, gender identity or expression, political beliefs or disability. If you need help with reading, writing, hearing, etc., under the Americans with Disabilities Act, you are invited to make your needs known to a DHS office in your area.
AUTHORITY: MCLA 400.9 |
COMPLETION: Voluntary |
A. H. Approval
Yes
No Date: