Form 032 02 0147 01 Eng is the form you use to declare your intention to work in the United States. This form is used by both citizens and non-citizens who want to work in the United States. It is important that you complete this form accurately and submit it to the appropriate government office. Failure to do so may result in delays or even deportation. Make sure you understand all of the requirements for Form 032 02 0147 01 Eng before submitting it.
| Question | Answer |
|---|---|
| Form Name | Form 032 02 0147 01 Eng |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | 032 02 0147 01 eng application for adult medical assistance virginia form |
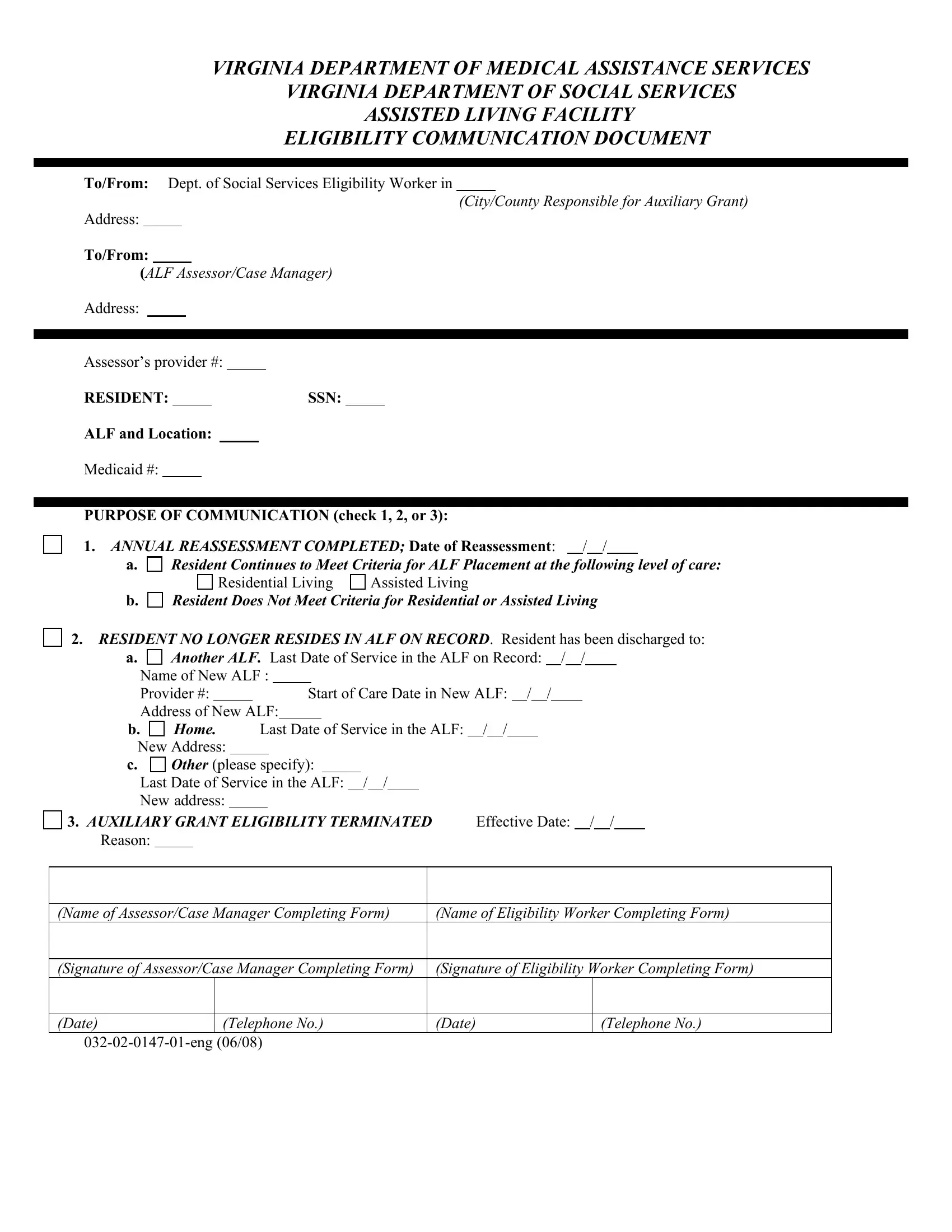
VIRGINIA DEPARTMENT OF MEDICAL ASSISTANCE SERVICES
VIRGINIA DEPARTMENT OF SOCIAL SERVICES
ASSISTED LIVING FACILITY
ELIGIBILITY COMMUNICATION DOCUMENT
TO/FROM: Dept. of Social Services Eligibility Worker in
(City/County Responsible for Auxiliary Grant)
Address:
TO/FROM:
(ALF Assessor/Case Manager)
Address:
Assessor’s provider #:
RESIDENT:SSN:
ALF AND LOCATION:
Medicaid #:
PURPOSE OF COMMUNICATION (CHECK 1, 2, OR 3):
1. ANNUAL REASSESSMENT COMPLETED; DATE OF REASSESSMENT: / /
A. |
Resident Continues to Meet Criteria for ALF Placement at the following level of care: |
|
|
Residential Living |
Assisted Living |
B. |
Resident Does Not Meet Criteria for Residential or Assisted Living |
|
2.RESIDENT NO LONGER RESIDES IN ALF ON RECORD. Resident has been discharged to:
A. |
Another ALF. Last Date of Service in the ALF on Record: |
/ |
/ |
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||
Name of New ALF : |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
Provider #: |
|
|
|
|
|
Start of Care Date in New ALF: / |
/ |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Address of New ALF: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
B. |
Home. |
Last Date of Service in the ALF: / / |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
New Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
C. |
Other (please specify): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
Last Date of Service in the ALF: / / |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
New address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
3. AUXILIARY GRANT ELIGIBILITY TERMINATED |
|
Effective Date: |
/ / |
|
|
|||||||||||||||||||||||||||||||||||||
Reason: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||
(Name of Assessor/Case Manager Completing Form) |
|
(Name of Eligibility Worker Completing Form) |
||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||
(Signature of Assessor/Case Manager Completing Form) |
|
(Signature of Eligibility Worker Completing Form) |
||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
(Date) |
|
|
(Telephone No.) |
|
(Date) |
|
|
|
|
|
|
|
|
(Telephone No.) |
||||||||||||||||||||||||||||
ALF ELIGIBILITY COMMUNICATION DOCUMENT INSTRUCTIONS
WHEN TO USE THIS FORM
This form is a communication tool between the local department of social services (LDSS) eligibility worker, the assessor/case manager responsible for the
1.The assessor to the eligibility worker and to DMAS at the time of a
2.Either the assessor or eligibility worker to the other and to DMAS whenever either becomes aware of a change in address; and
3.The eligibility worker to the ALF assessor and to DMAS whenever the AG is terminated.
TO/FROM SECTION
Both TO/FROM sections must be completed. Completely fill in the locality of the DSS eligibility worker with address and indicate whether document is to be sent to or from the eligibility worker by circling “TO” or “FROM.” In the second TO/FROM section, completely fill in the assessor’s name, address and provider number and indicate whether the document is to be sent to or from the assessor or case manager by circling “TO” or “FROM.”
RESIDENT IDENTIFICATION SECTION
1.RESIDENT: Legibly print name of ALF resident who is being assessed, who has moved, or whose AG has been terminated.
2.SSN: Write in the resident’s social security number.
3.ALF: Legibly print the name of the ALF in which the resident resides.
4.ALF location: List the city/town in which the ALF is located.
5.Medicaid Number: Write in the resident’s Medicaid number.
PURPOSE OF COMMUNICATION SECTION: Check either 1, 2, or 3.
IF 1 IS CHECKED: (Annual Reassessment Completed), fill in the date of the reassessment. Check either a. (Resident continues to meet criteria for ALF placement at the following level of care) or b. (Resident does not meet criteria for residential or assisted living. If a. is checked, indicate which level of care the individual meets. If intensive assisted living is checked, respond to the two questions “continues to need intensive assisted living services” and “based on the UAI, continues to meet criteria for intensive assisted living.” Usually, both will be checked “yes.” When 1. is checked, the assessor sends a copy of the Uniform Assessment Instrument (UAI), the ALF Eligibility Communication Document (ECD), and the
NOTE: If a reassessment indicates a change in level of care, treat the assessment as a change in level of care. That is, send a copy of the UAI and the
IF 2 IS CHECKED: (Resident no longer resides in ALF on record), indicate to where the resident moved (i.e., another ACR, home, or other). For each, indicate the last date of service in the ALF on record. Complete other information such as new address, etc., if known. When 2 is checked, the assessor/case manager or eligibility worker completing the ECD should send a copy to the other and a copy to DMAS and keep a copy for him- or herself.
IF 3 IS CHECKED: (Auxiliary Grant Eligibility Terminated), the eligibility worker indicates the effective date of termination and the reason. Then the eligibility worker sends a copy of the ECD to the assessor/case manager and to DMAS.
SIGNATURES SECTION
For each form completed, only one signature section will be completed. For example, if an assessor is completing the form for a reassessment, the
Please photocopy this form as needed; plain paper copies are acceptable.