
Form 107 003 can be filled out with ease. Simply open FormsPal PDF editor to finish the job in a timely fashion. FormsPal team is dedicated to making sure you have the best possible experience with our tool by consistently adding new functions and enhancements. Our editor has become even more useful thanks to the most recent updates! Now, filling out documents is simpler and faster than before. Starting is effortless! All that you should do is take these easy steps below:
Step 1: Click on the orange "Get Form" button above. It's going to open our tool so that you could begin filling in your form.
Step 2: As you access the file editor, you will find the document all set to be completed. Other than filling in different blanks, you may also perform various other actions with the file, such as adding custom text, editing the initial textual content, adding illustrations or photos, affixing your signature to the form, and a lot more.
With regards to the fields of this particular document, this is what you need to do:
1. Fill out your Form 107 003 with a number of essential blanks. Collect all the information you need and make sure not a single thing omitted!
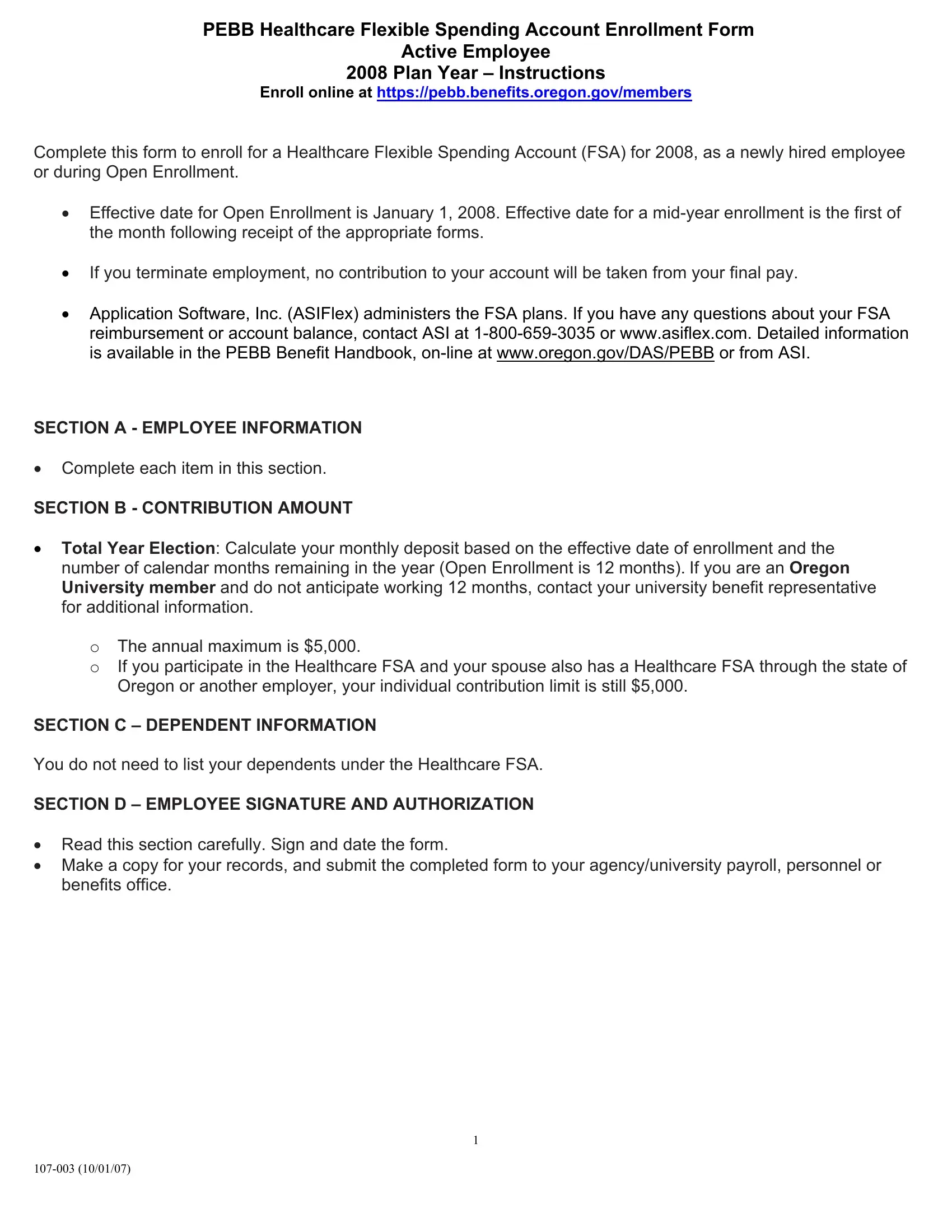
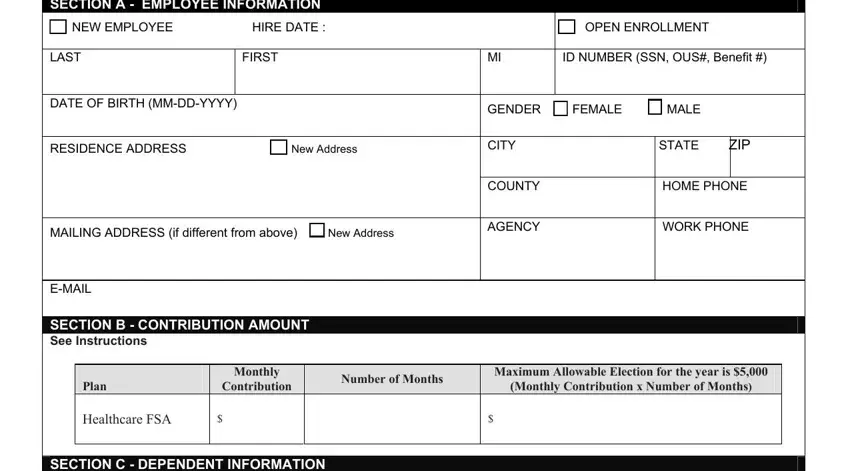
2. The third stage is to fill in the following blanks: SECTION A EMPLOYEE INFORMATION, OPEN ENROLLMENT, LAST, FIRST, ID NUMBER SSN OUS Benefit, DATE OF BIRTH MMDDYYYY, RESIDENCE ADDRESS New Address, MAILING ADDRESS if different from, SECTION B CONTRIBUTION AMOUNT See, GENDER FEMALE MALE, CITY, STATE, ZIP, COUNTY, and HOME PHONE.
Always be really careful while completing FIRST and GENDER FEMALE MALE, because this is the part where most users make mistakes.
3. Completing I have read the PEBB Benefit, Approved By initial Date Approved, and PEBB Use Only is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
Step 3: Make sure that your information is right and then simply click "Done" to proceed further. Join FormsPal now and immediately get access to Form 107 003, set for downloading. All changes made by you are preserved , enabling you to customize the pdf later when necessary. Here at FormsPal.com, we do everything we can to make certain that all of your information is maintained protected.