Form Ac 916 is an important form to be familiar with if you are a business owner. This form is used for reporting payments made to vendors, and it must be filed on a quarterly basis. Knowing how to complete this form correctly can help you stay compliant with tax laws and ensure that your business records are accurate. In this blog post, we will walk you through the basics of Form Ac 916 so that you can understand how to accurately complete it. We will also provide some tips on ensuring that your business stays compliant with tax laws in regards to vendor payments. Thanks for reading!
| Question | Answer |
|---|---|
| Form Name | Form Ac 916 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | Comptroller, Accum, Payees, Orig |
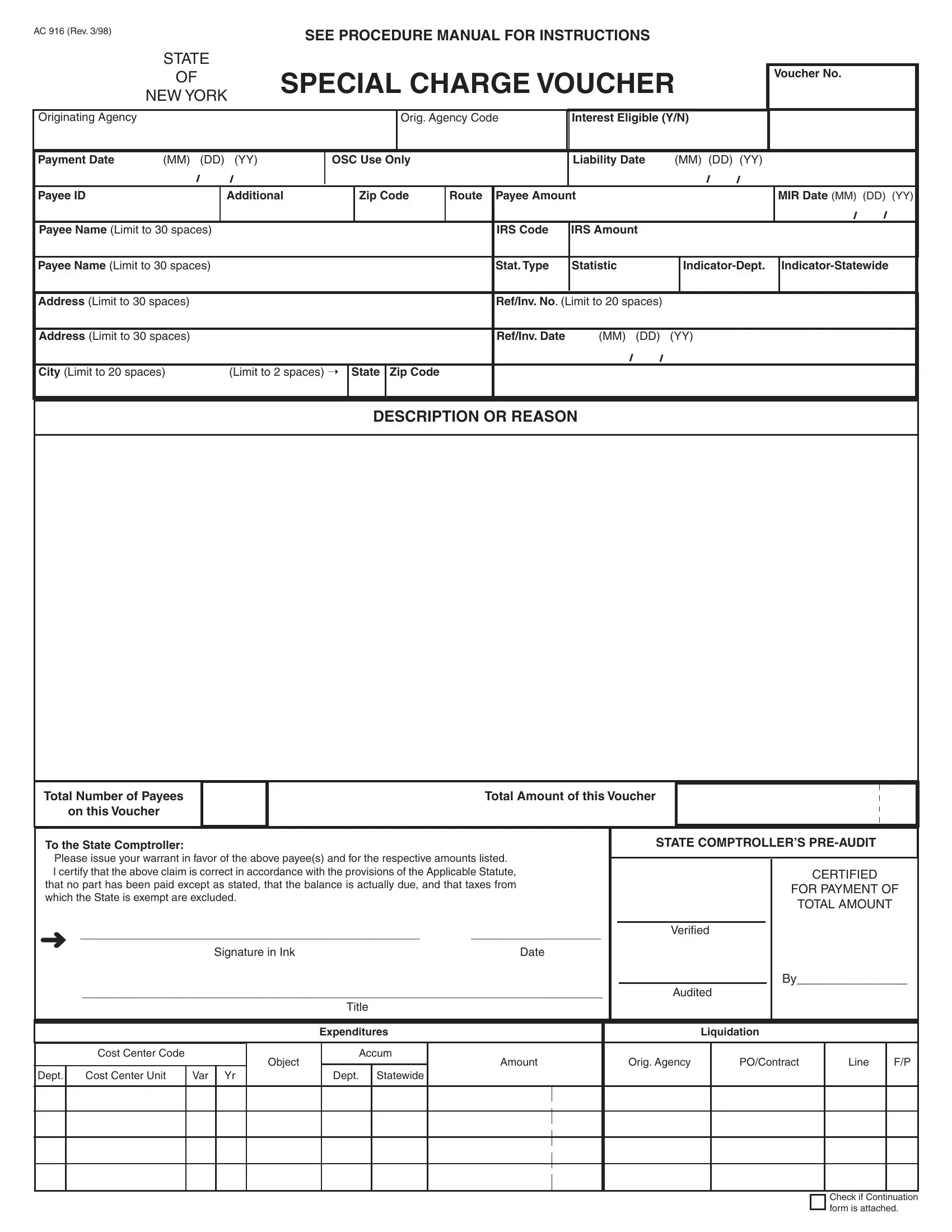
AC 916 (Rev. 3/98)
SEE PROCEDURE MANUAL FOR INSTRUCTIONS
STATE
OFSPECIAL CHARGE VOUCHER
NEW YORK
Voucher No.
Originating Agency
Orig. Agency Code
Interest Eligible (Y/N)
Payment Date |
(MM) (DD) (YY) |
OSC Use Only
Liability Date |
(MM) (DD) (YY) |
Payee ID
Additional
Zip Code
Route
Payee Amount
MIR Date (MM) (DD) (YY)
Payee Name (Limit to 30 spaces)
IRS Code
IRS Amount
Payee Name (Limit to 30 spaces)
Stat. Type
Statistic
Address (Limit to 30 spaces)
Ref/Inv. No. (Limit to 20 spaces)
Address (Limit to 30 spaces)
Ref/Inv. Date |
(MM) (DD) (YY) |
City (Limit to 20 spaces) |
(Limit to 2 spaces) Ý |
State Zip Code
DESCRIPTION OR REASON
Total Number of Payees
on this Voucher
Total Amount of this Voucher
To the State Comptroller:
Please issue your warrant in favor of the above payee(s) and for the respective amounts listed.
I certify that the above claim is correct in accordance with the provisions of the Applicable Statute, that no part has been paid except as stated, that the balance is actually due, and that taxes from which the State is exempt are excluded.
Ü______________________________________________________________________________________
Signature in InkDate
______________________________________________________________________________________
Title
STATE COMPTROLLER’S
CERTIFIED
FOR PAYMENT OF
TOTAL AMOUNT
Verified
By________________
Audited
|
|
|
|
|
Expenditures |
|
Liquidation |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cost Center Code |
|
|
Object |
Accum |
Amount |
Orig. Agency |
|
PO/Contract |
Line |
F/P |
|
|
|
|
|
|
|
|
||||||
Dept. |
Cost Center Unit |
Var |
Yr |
|
Dept. |
Statewide |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Check if Continuation form is attached.