Form Bhcs Ltc 125 is a discontinued circuit breaker that was manufactured by the Federal Pacific Electric Company. It is a 125 amp, 240 volt, 3-pole breaker that is UL approved. The Form Bhcs Ltc 125 has been discontinued and is no longer in production. However, it may still be available for purchase from some suppliers. If you are looking for a replacement for your Form Bhcs Ltc 125 breaker, there are several similar options that are currently available. One such option is the Square D QO125FA Circuit Breaker, which is also a 125 amp, 240 volt breaker that is UL approved. Another option would be the Siemens TE1125AF3BUL125U Breaker, which again is a 125 amp, 240 volt breaker with an elevated interrupt rating. Whether you are looking to replace your current Form Bhcs Ltc 125 breaker or are just researching different options, we hope this article provides some helpful information. Thank you for reading!
| Question | Answer |
|---|---|
| Form Name | Form Bhcs Ltc 125 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | licensure, remit, REGULATORY, 1978 |
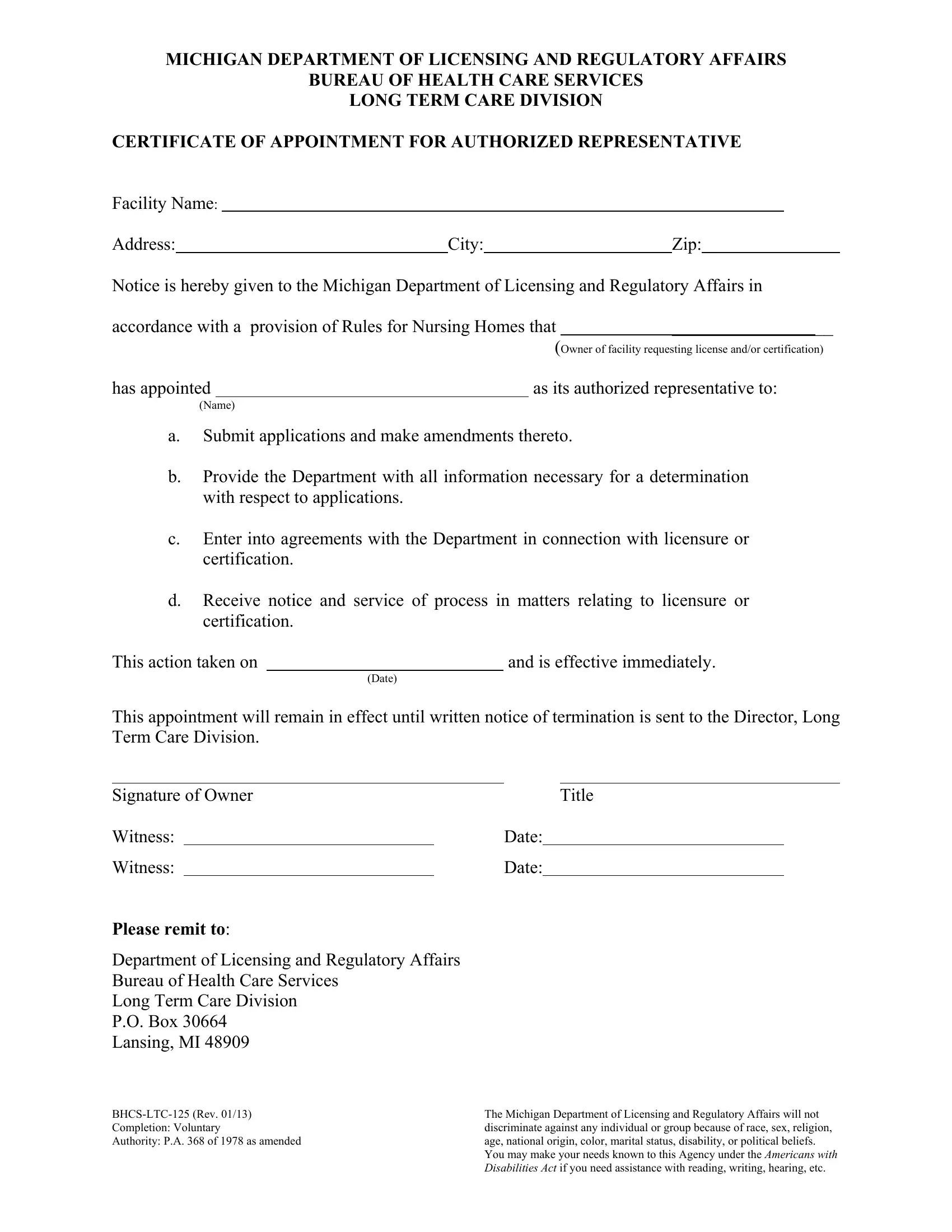
MICHIGAN DEPARTMENT OF LICENSING AND REGULATORY AFFAIRS
BUREAU OF HEALTH CARE SERVICES
LONG TERM CARE DIVISION
CERTIFICATE OF APPOINTMENT FOR AUTHORIZED REPRESENTATIVE
Facility Name:
Address: |
|
City: |
Zip: |
||||||
|
|
|
|
|
|
|
|
|
|
Notice is hereby given to the Michigan Department of Licensing and Regulatory Affairs in |
|||||||||
accordance with a provision of Rules for Nursing Homes that |
|
__________________ |
|||||||
|
|
|
|
|
|
|
|
||
|
|
|
|
|
(Owner of facility requesting license and/or certification) |
||||
has appointed |
|
|
|
as its authorized representative to: |
|||||
|
(Name) |
|
|
|
|
|
|
|
|
a.Submit applications and make amendments thereto.
b.Provide the Department with all information necessary for a determination with respect to applications.
c.Enter into agreements with the Department in connection with licensure or certification.
d.Receive notice and service of process in matters relating to licensure or certification.
This action taken on |
|
and is effective immediately. |
|
(Date) |
|
This appointment will remain in effect until written notice of termination is sent to the Director, Long Term Care Division.
Signature of Owner |
Title |
Witness:Date:
Witness:Date:
PLEASE REMIT TO:
Department of Licensing and Regulatory Affairs
Bureau of Health Care Services
Long Term Care Division
P.O. Box 30664
Lansing, MI 48909
The Michigan Department of Licensing and Regulatory Affairs will not |
|
Completion: Voluntary |
discriminate against any individual or group because of race, sex, religion, |
Authority: P.A. 368 of 1978 as amended |
age, national origin, color, marital status, disability, or political beliefs. |
|
You may make your needs known to this Agency under the AMERICANS WITH |
|
DISABILITIES ACT if you need assistance with reading, writing, hearing, etc. |