The City of Calgary's Community Services Department has released Form Ccl 009, which outlines the rules and regulations for filming in public areas. This form is for anyone who wishes to film in a public area within the city, including commercial and private filmmakers, news crews, and hobbyists. Filming in a public place can be a great way to capture memories or share your story with others, but it's important to know what restrictions apply so that you don't run into any problems. The City of Calgary has created this form to help clarify the rules and make the process easier for everyone involved. If you're planning on filming in a public area, be sure to read through this form carefully and contact the Community Services Department if you have any questions.
| Question | Answer |
|---|---|
| Form Name | Form Ccl 009 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | CCL_009_Health_ Assessment_16_ _Older department of aging form kansas how to fill out form |
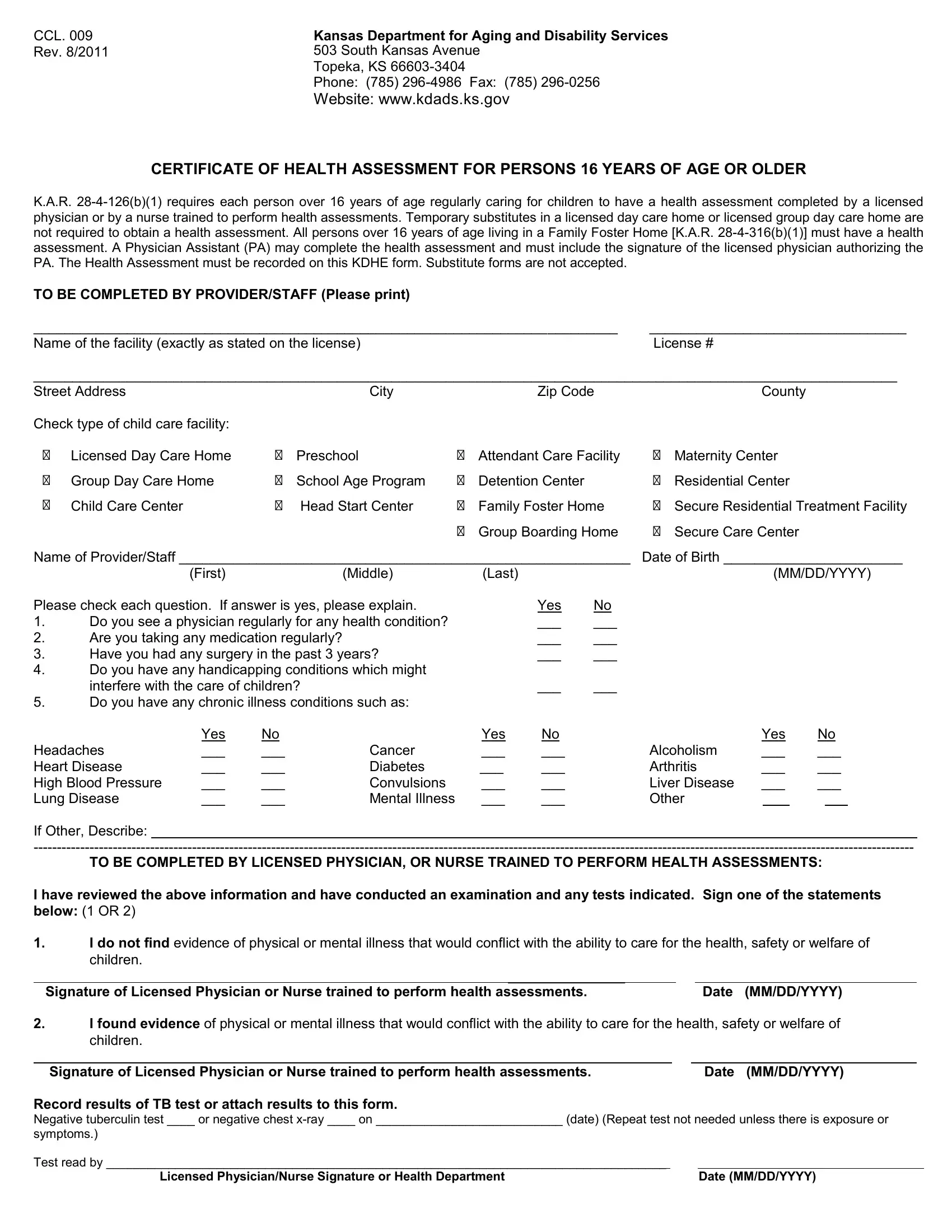
CCL. 009 Rev. 8/2011
Kansas Department for Aging and Disability Services 503 South Kansas Avenue
Topeka, KS
Phone: (785)
Website: www.kdads.ks.gov
CERTIFICATE OF HEALTH ASSESSMENT FOR PERSONS 16 YEARS OF AGE OR OLDER
K.A.R.
TO BE COMPLETED BY PROVIDER/STAFF (Please print) |
|
___________________________________________________________________________ |
_________________________________ |
Name of the facility (exactly as stated on the license) |
License # |
_______________________________________________________________________________________________________________
Street Address |
|
City |
|
Zip Code |
|
County |
Check type of child care facility: |
|
|
|
|
|
|
Licensed Day Care Home |
Preschool |
Attendant Care Facility |
Maternity Center |
|||
Group Day Care Home |
School Age Program |
Detention Center |
Residential Center |
|||
Child Care Center |
Head Start Center |
Family Foster Home |
Secure Residential Treatment Facility |
|||
|
|
|
Group Boarding Home |
Secure Care Center |
||
Name of Provider/Staff __________________________________________________________ Date of Birth _______________________
|
(First) |
(Middle) |
(Last) |
|
(MM/DD/YYYY) |
Please check each question. If answer is yes, please explain. |
|
Yes |
No |
||
1. |
Do you see a physician regularly for any health condition? |
|
___ |
___ |
|
2. |
Are you taking any medication regularly? |
|
|
___ |
___ |
3. |
Have you had any surgery in the past 3 years? |
|
___ |
___ |
|
4.Do you have any handicapping conditions which might
interfere with the care of children? |
___ |
___ |
5.Do you have any chronic illness conditions such as:
|
Yes |
No |
|
Yes |
No |
|
Yes |
No |
||
Headaches |
___ |
___ |
Cancer |
___ |
___ |
Alcoholism |
___ |
___ |
||
Heart Disease |
___ |
___ |
Diabetes |
___ |
___ |
Arthritis |
___ |
___ |
||
High Blood Pressure |
___ |
___ |
Convulsions |
___ |
___ |
Liver Disease |
___ |
___ |
||
Lung Disease |
___ |
___ |
Mental Illness |
___ |
___ |
Other |
|
|
|
|
If Other, Describe:____
TO BE COMPLETED BY LICENSED PHYSICIAN, OR NURSE TRAINED TO PERFORM HEALTH ASSESSMENTS:
I have reviewed the above information and have conducted an examination and any tests indicated. Sign one of the statements below: (1 OR 2)
1.I do not find evidence of physical or mental illness that would conflict with the ability to care for the health, safety or welfare of children.
_______________ |
|
|
Signature of Licensed Physician or Nurse trained to perform health assessments. |
|
Date (MM/DD/YYYY) |
2.I found evidence of physical or mental illness that would conflict with the ability to care for the health, safety or welfare of
children. |
|
|
|
________________________ |
_ |
|
|
Signature of Licensed Physician or Nurse trained to perform health assessments. |
|
|
Date (MM/DD/YYYY) |
Record results of TB test or attach results to this form.
Negative tuberculin test ____ or negative chest
symptoms.)
Test read by _________________________________________________________________________________ |
|
Licensed Physician/Nurse Signature or Health Department |
Date (MM/DD/YYYY) |