The Department of Public Health's Form CDPH 8435 is used to request specific information from medical facilities. The form is most commonly used to request mortality data, but it can also be used to request other types of information. The instructions for filling out the form are clear and concise, making it easy to complete. If you need any additional assistance, the DPH website has a wealth of resources that can help you.
| Question | Answer |
|---|---|
| Form Name | Form Cdph 8435 Sra |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | rhb, nonrefundable, cdph8435sra3, Radiologic |
State of |
California Department of Public Health |
|
Radiologic Health Branch |
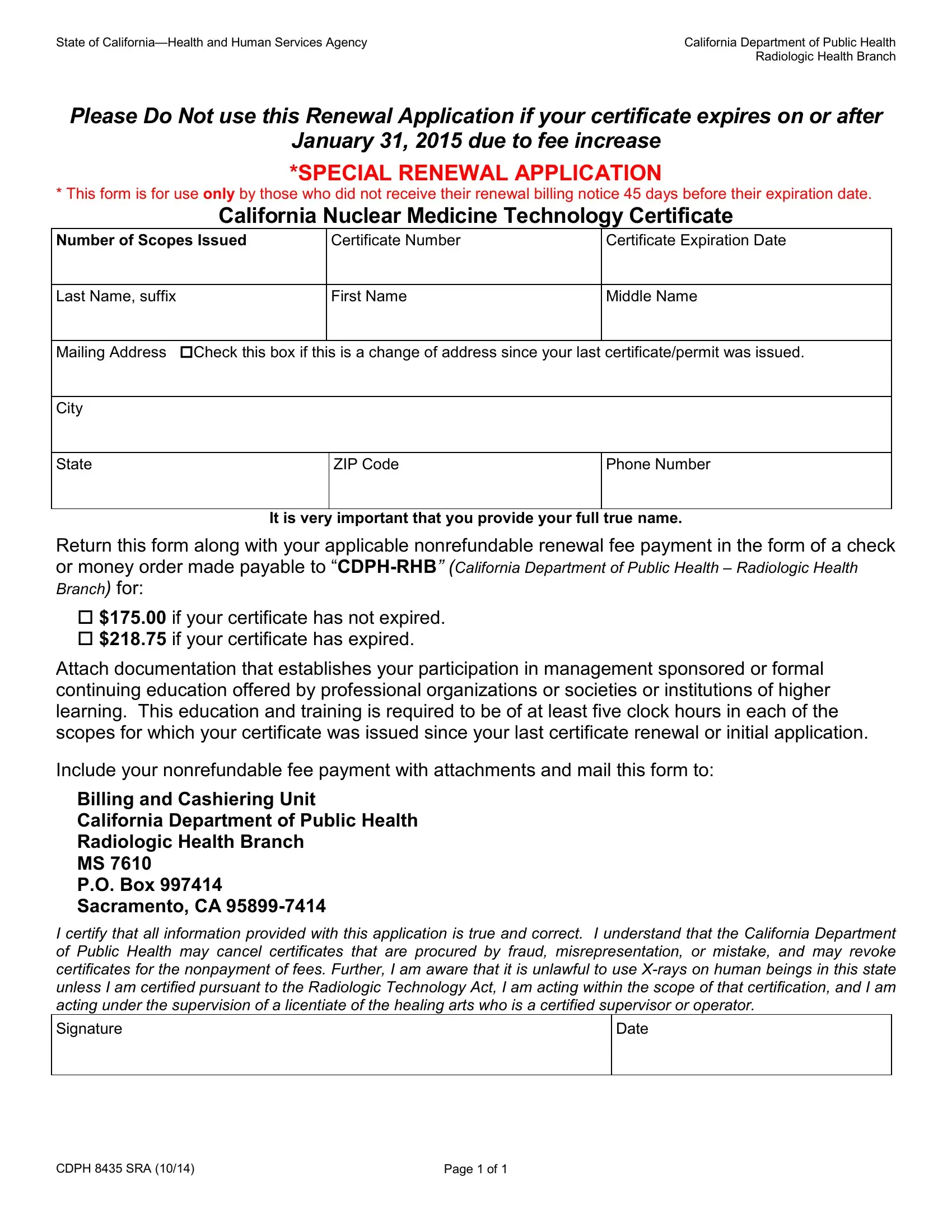
Please Do Not use this Renewal Application if your certificate expires on or after
January 31, 2015 due to fee increase
*SPECIAL RENEWAL APPLICATION
* This form is for use only by those who did not receive their renewal billing notice 45 days before their expiration date.
California Nuclear Medicine Technology Certificate
Number of Scopes Issued |
Certificate Number |
Certificate Expiration Date |
|
|
|
Last Name, suffix |
First Name |
Middle Name |
|
|
|
Mailing Address Check this box if this is a change of address since your last certificate/permit was issued.
City
State
ZIP Code
Phone Number
It is very important that you provide your full true name.
Return this form along with your applicable nonrefundable renewal fee payment in the form of a check
or money order made payable to
$175.00 if your certificate has not expired.
$218.75 if your certificate has expired.
Attach documentation that establishes your participation in management sponsored or formal continuing education offered by professional organizations or societies or institutions of higher learning. This education and training is required to be of at least five clock hours in each of the scopes for which your certificate was issued since your last certificate renewal or initial application.
Include your nonrefundable fee payment with attachments and mail this form to:
Billing and Cashiering Unit
California Department of Public Health
Radiologic Health Branch
MS 7610
P.O. Box 997414
Sacramento, CA
I certify that all information provided with this application is true and correct. I understand that the California Department of Public Health may cancel certificates that are procured by fraud, misrepresentation, or mistake, and may revoke certificates for the nonpayment of fees. Further, I am aware that it is unlawful to use
Signature
Date
CDPH 8435 SRA (10/14) |
Page 1 of 1 |