
You'll be able to fill out USGLI instantly with the help of our online editor for PDFs. Our development team is relentlessly working to enhance the tool and make it even better for people with its multiple functions. Enjoy an ever-evolving experience now! For anyone who is seeking to get started, this is what it requires:
Step 1: First, open the pdf tool by clicking the "Get Form Button" above on this page.
Step 2: When you open the online editor, you will find the document prepared to be filled out. Besides filling in various blanks, you can also do various other things with the form, namely putting on custom textual content, editing the initial text, adding images, signing the document, and much more.
This form needs specific details; in order to ensure consistency, be sure to adhere to the next steps:
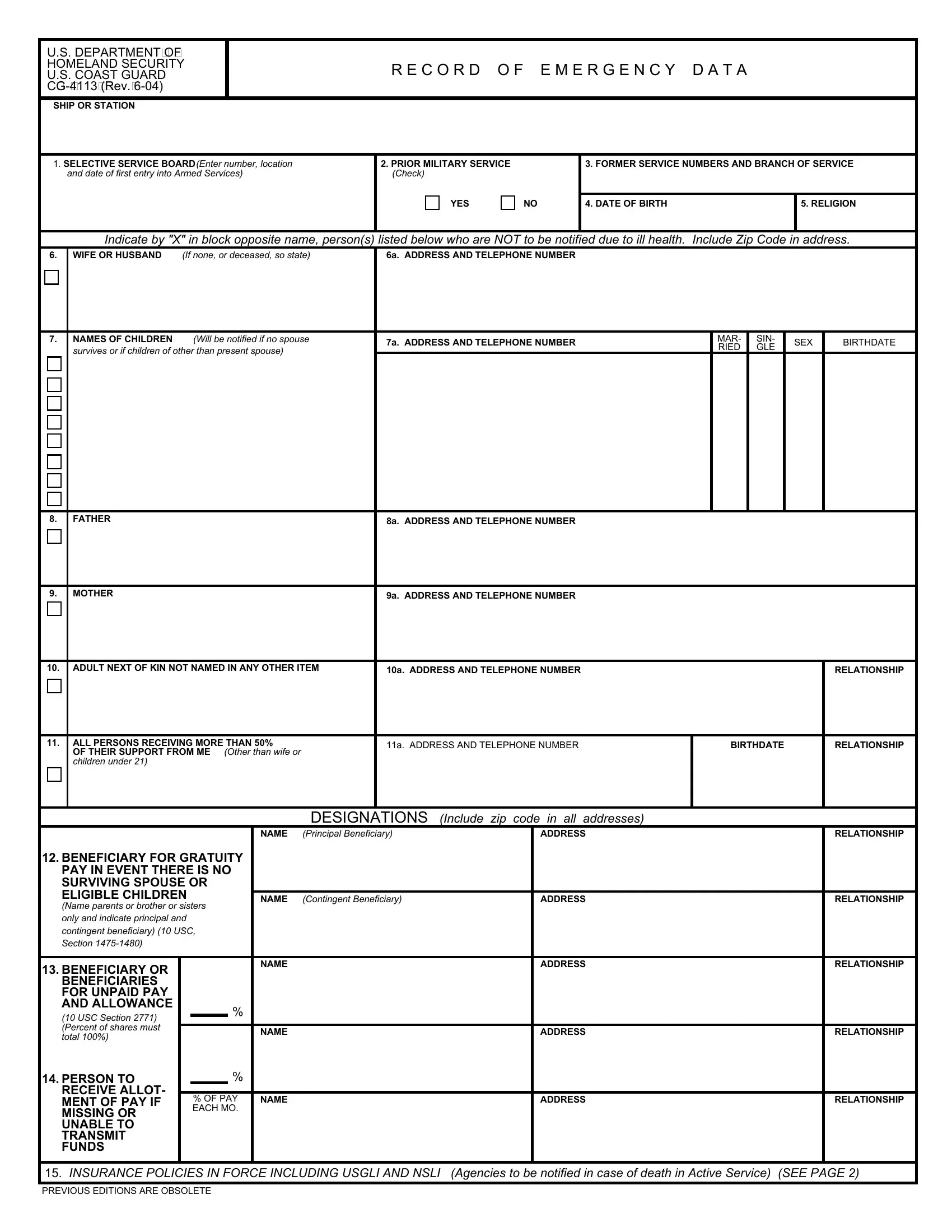
1. Start filling out the USGLI with a group of major fields. Collect all the required information and be sure absolutely nothing is forgotten!
2. Once the previous segment is finished, you have to put in the essential details in MOTHER, a ADDRESS AND TELEPHONE NUMBER, ADULT NEXT OF KIN NOT NAMED IN, a ADDRESS AND TELEPHONE NUMBER, RELATIONSHIP, ALL PERSONS RECEIVING MORE THAN, OF THEIR SUPPORT FROM ME children, Other than wife or, a ADDRESS AND TELEPHONE NUMBER, BIRTHDATE, RELATIONSHIP, DESIGNATIONS Include zip code in, ADDRESS, NAME, and RELATIONSHIP so you're able to proceed to the third part.
3. Your next stage is going to be straightforward - fill out all the empty fields in BENEFICIARY OR BENEFICIARIES FOR, PERSON TO, RECEIVE ALLOT MENT OF PAY IF, NAME, OF PAY EACH MO, NAME, ADDRESS, ADDRESS, RELATIONSHIP, RELATIONSHIP, and INSURANCE POLICIES IN FORCE to conclude the current step.
4. It's time to fill out this fourth part! In this case you'll have these INSURANCE POLICIES IN FORCE, SGLI, SGLI, SGLI, SGLI, SGLI, SGLI, SGLI, SGLI, SGLI, SGLI, NOT PARTICIPATING, FULL NAME AND ADDRESS OF COMPANY, ADDRESS OF OFFICE RECEIVING, and POLICY NUMBER empty form fields to fill out.
5. This document must be finished by going through this area. Further you will see a detailed listing of fields that need correct information for your form usage to be accomplished: NAME OF DESIGNATOR, Last first middle, PRESENT SERVICE NO, GRADERATE, SOCIAL SECURITY NUMBER, PRIVACY ACT STATEMENT, In accordance with USC ae the, AUTHORITY which authorizes the, PRINCIPAL PURPOSES for which, Persons to receive death gratuity, or death Persons to receive, ROUTINE USES which may be made of, eligible to receive benefits as, DISCLOSURE of the information is, and the next of kin of a casualty in a.
Be extremely careful when filling out AUTHORITY which authorizes the and PRINCIPAL PURPOSES for which, since this is the part where a lot of people make errors.
Step 3: Revise all the information you've typed into the form fields and click on the "Done" button. Get your USGLI after you sign up for a 7-day free trial. Immediately gain access to the form inside your FormsPal account page, along with any modifications and changes automatically saved! Here at FormsPal, we endeavor to be sure that all your information is kept private.