Form CG 6100 is an application used to apply for a Certificate of Good Standing from the California Secretary of State. The form is used by business entities registered in California, such as corporations and limited liability companies, to prove that they are in good standing with the state. The certificate issued by the Secretary of State confirms that the company is in compliance with all state laws and regulations. completing Form CG 6100 is easy - just follow these simple steps! If your business entity is registered in California, you may need to apply for a Certificate of Good Standing from the Secretary of State. Form CG 6100 is the application used for this purpose. The certificate proves that your company is in good standing with the state and compliant with all applicable laws and regulations. Completing Form CG 6100 is easy - just follow these simple steps!
| Question | Answer |
|---|---|
| Form Name | Form Cg 6100 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | cg 6100 form, 1974, HCG, chemoprophylaxis |
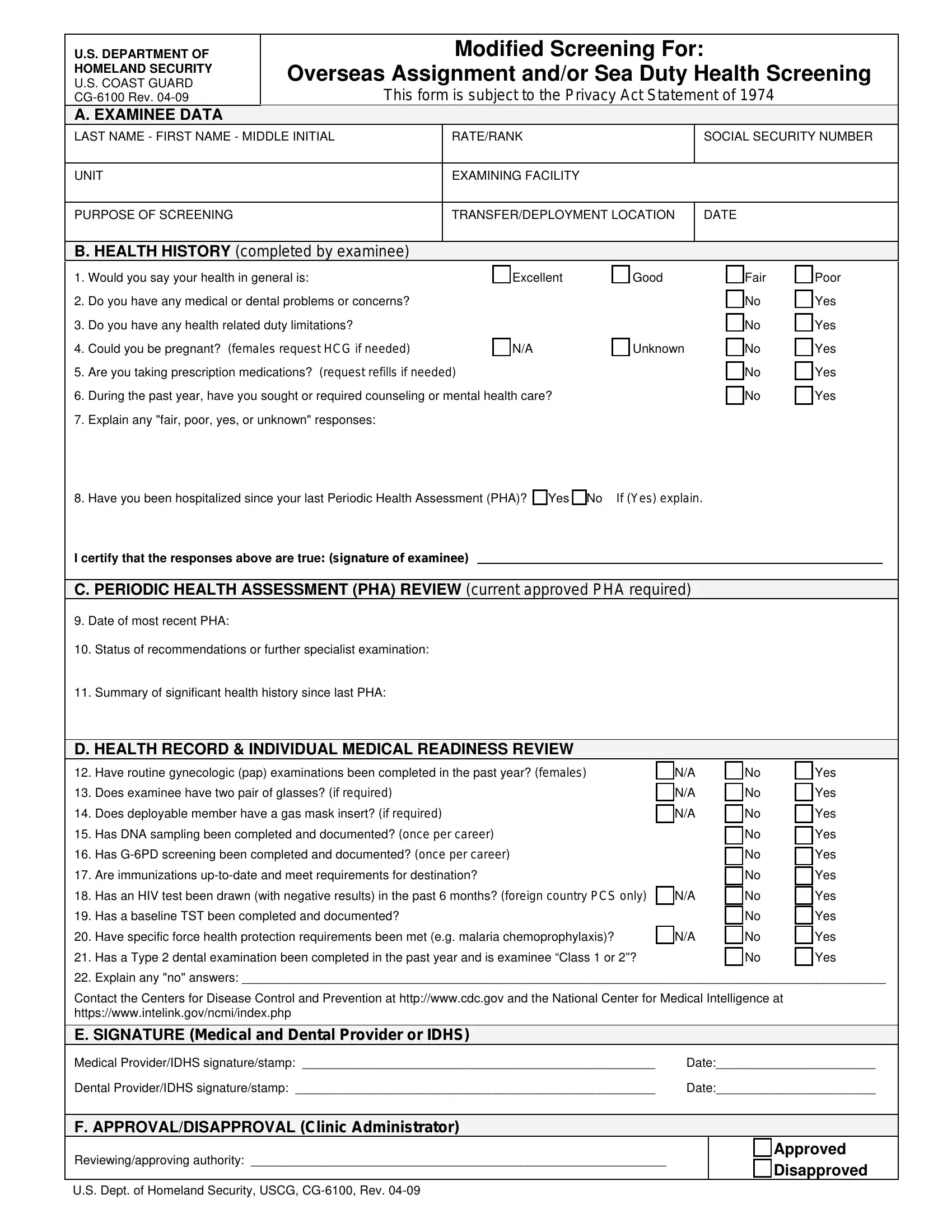
U.S. DEPARTMENT OF |
|
|
Modified Screening For: |
|
|
||
HOMELAND SECURITY |
Overseas Assignment and/or Sea Duty Health Screening |
|
|||||
U.S. COAST GUARD |
|
||||||
|
This form is subject to the Privacy Act Statement of 1974 |
|
|||||
|
|
||||||
|
A. EXAMINEE DATA |
|
|
|
|
|
|
LAST NAME - FIRST NAME - MIDDLE INITIAL |
|
RATE/RANK |
|
SOCIAL SECURITY NUMBER |
|
||
|
|
|
|
|
|
|
|
UNIT |
|
|
EXAMINING FACILITY |
|
|
||
|
|
|
|
|
|
||
PURPOSE OF SCREENING |
|
|
TRANSFER/DEPLOYMENT LOCATION |
|
DATE |
|
|
|
|
|
|
|
|
|
|
B. HEALTH HISTORY (completed by examinee)
1. |
Would you say your health in general is: |
Excellent |
Good |
|
Fair |
Poor |
|
|
|||||
2. |
Do you have any medical or dental problems or concerns? |
|
|
|
No |
Yes |
|
|
|||||
3. |
Do you have any health related duty limitations? |
|
|
|
No |
Yes |
|
|
|||||
4. |
Could you be pregnant? (females request HCG if needed) |
N/A |
Unknown |
No |
Yes |
|
|
||||||
5. |
Are you taking prescription medications? (request refills if needed) |
|
|
|
No |
Yes |
|
|
|||||
6. |
During the past year, have you sought or required counseling or mental health care? |
|
|
No |
Yes |
|
|
||||||
7. |
Explain any "fair, poor, yes, or unknown" responses: |
|
|
|
|
|
|
|
|
||||
8. |
Have you been hospitalized since your last Periodic Health Assessment (PHA)? Yes No |
If (Yes) explain. |
|
|
|
|
|
||||||
|
I certify that the responses above are true: (signature of examinee) |
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C. PERIODIC HEALTH ASSESSMENT (PHA) REVIEW (current approved PHA required) |
|
|
|
|
|
||||||
9. |
Date of most recent PHA: |
|
|
|
|
|
|
|
|
||||
10. |
Status of recommendations or further specialist examination: |
|
|
|
|
|
|
|
|
||||
11. |
Summary of significant health history since last PHA: |
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
||||
|
|
D. HEALTH RECORD & INDIVIDUAL MEDICAL READINESS REVIEW |
|
|
|
|
|
|
|
||||
12. |
Have routine gynecologic (pap) examinations been completed in the past year? (females) |
|
N/A |
No |
Yes |
|
|
||||||
13. |
Does examinee have two pair of glasses? (if required) |
|
|
N/A |
No |
Yes |
|
|
|||||
14. |
Does deployable member have a gas mask insert? (if required) |
|
|
N/A |
No |
Yes |
|
|
|||||
15. |
Has DNA sampling been completed and documented? (once per career) |
|
|
|
No |
Yes |
|
|
|||||
16. |
Has |
|
|
|
No |
Yes |
|
|
|||||
17. |
Are immunizations |
|
|
|
No |
Yes |
|
|
|||||
18. |
Has an HIV test been drawn (with negative results) in the past 6 months? (foreign country PCS only) |
N/A |
No |
Yes |
|
|
|||||||
19. |
Has a baseline TST been completed and documented? |
|
|
|
No |
Yes |
|
|
|||||
20. |
Have specific force health protection requirements been met (e.g. malaria chemoprophylaxis)? |
|
N/A |
No |
Yes |
|
|
||||||
21. |
Has a Type 2 dental examination been completed in the past year and is examinee “Class 1 or 2”? |
|
No |
Yes |
|
|
|||||||
22. |
Explain any "no" answers: _____________________________________________________________________________________________ |
|
|
||||||||||
|
Contact the Centers for Disease Control and Prevention at http://www.cdc.gov and the National Center for Medical Intelligence at |
|
|
||||||||||
|
https://www.intelink.gov/ncmi/index.php |
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
E. SIGNATURE (Medical and Dental Provider or IDHS) |
|
|
|
|
|
|
|
|
|||
|
Medical Provider/IDHS signature/stamp: ___________________________________________________ |
Date:_______________________ |
|
|
|||||||||
|
Dental Provider/IDHS signature/stamp: ____________________________________________________ |
Date:_______________________ |
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
F. APPROVAL/DISAPPROVAL (Clinic Administrator) |
|
|
|
|
|
|
|
|
|||
|
Reviewing/approving authority: ____________________________________________________________ |
|
|
Approved |
|
|
|||||||
|
|
|
Disapproved |
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
||
U.S. Dept. of Homeland Security, USCG,