This form is for requesting a change to your state income tax withholding. The purpose of this form is to request that more or less money be withheld from your paychecks for state income tax. You may use this form if you would like to have more or less money withheld than the amount shown on your most recent wage and tax statement, W-2. Use Form Cs3 to request any changes in withholding you would like to make, including a change in the number of exemptions you claim. If you are married and filing jointly, both spouses should complete a separate Form Cs3. Be sure to include your Social Security number and signature on the form. You can submit the form electronically or by mail. For more information, visit our website at www.taxadmin.org/fta/forms/cs3_instructions.pdf . Form Cs3 can be used to make desired adjustments in state income tax withholdings without waiting until filing season when changes could result in monetary penalties or even criminal charges against an individual taxp
| Question | Answer |
|---|---|
| Form Name | Form Cs3 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | incur, 15th, nis contribution schedule form cs3 forms, INSURABLE |
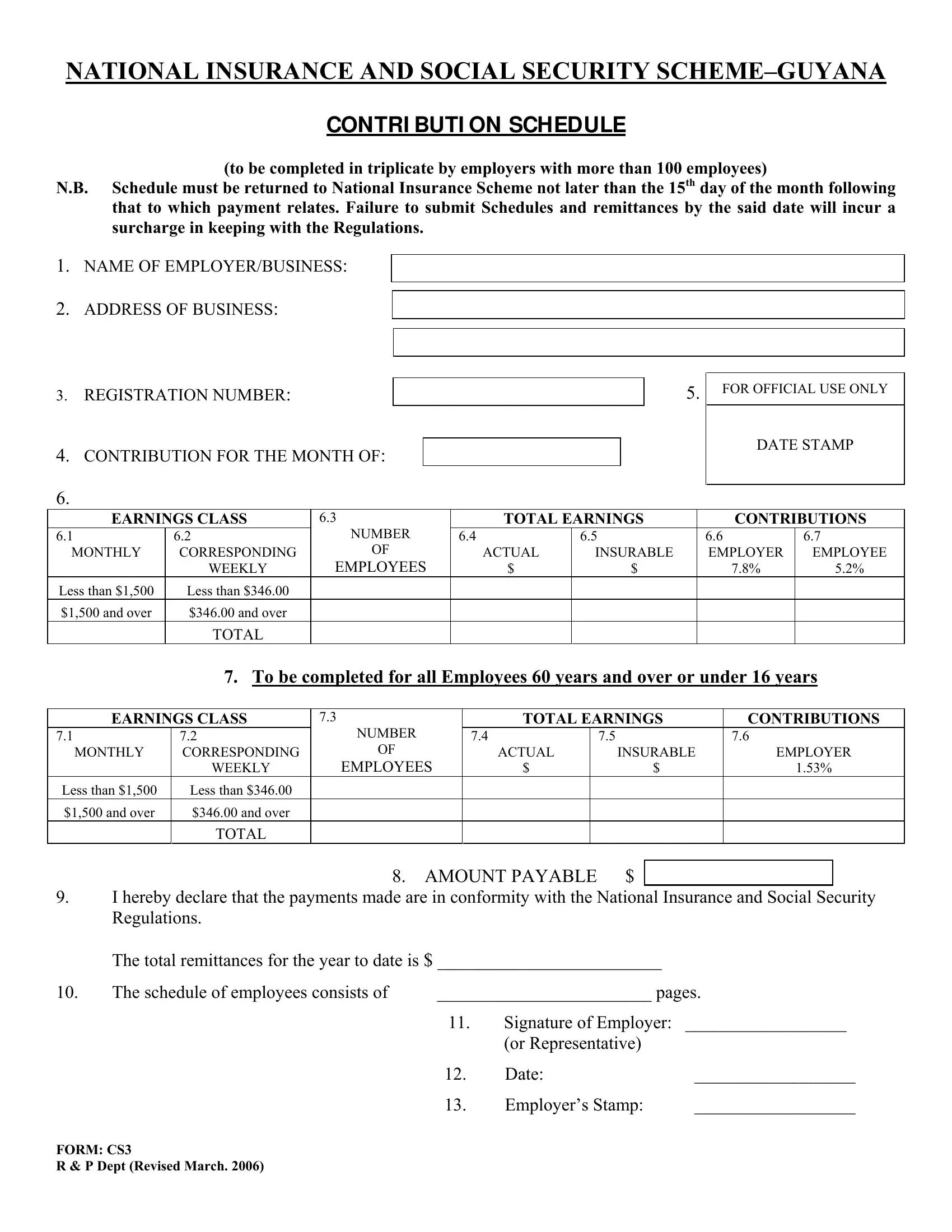
NATIONAL INSURANCE AND SOCIAL SECURITY
CONTRI BUTI ON SCHEDULE
(to be completed in triplicate by employers with more than 100 employees)
N.B. Schedule must be returned to National Insurance Scheme not later than the 15th day of the month following that to which payment relates. Failure to submit Schedules and remittances by the said date will incur a surcharge in keeping with the Regulations.
1.NAME OF EMPLOYER/BUSINESS:
2.ADDRESS OF BUSINESS:
3.REGISTRATION NUMBER:
4.CONTRIBUTION FOR THE MONTH OF:
5.
FOR OFFICIAL USE ONLY
DATE STAMP
6.
EARNINGS CLASS |
6.3 |
TOTAL EARNINGS |
CONTRIBUTIONS |
|||
6.1 |
6.2 |
NUMBER |
6.4 |
6.5 |
6.6 |
6.7 |
MONTHLY |
CORRESPONDING |
OF |
ACTUAL |
INSURABLE |
EMPLOYER |
EMPLOYEE |
|
WEEKLY |
EMPLOYEES |
$ |
$ |
7.8% |
5.2% |
Less than $1,500 |
Less than $346.00 |
|
|
|
|
|
$1,500 and over |
$346.00 and over |
|
|
|
|
|
|
TOTAL |
|
|
|
|
|
7.To be completed for all Employees 60 years and over or under 16 years
EARNINGS CLASS |
7.3 |
|
|
TOTAL EARNINGS |
CONTRIBUTIONS |
|||||
7.1 |
7.2 |
NUMBER |
|
7.4 |
|
|
7.5 |
|
7.6 |
|
MONTHLY |
CORRESPONDING |
OF |
|
|
ACTUAL |
|
INSURABLE |
EMPLOYER |
||
|
WEEKLY |
EMPLOYEES |
|
$ |
|
$ |
1.53% |
|
||
Less than $1,500 |
Less than $346.00 |
|
|
|
|
|
|
|
|
|
$1,500 and over |
$346.00 and over |
|
|
|
|
|
|
|
|
|
|
TOTAL |
|
|
|
|
|
|
|
|
|
|
|
8. |
AMOUNT PAYABLE |
$ |
|
|
|
|||
|
|
|
|
|
||||||
9.I hereby declare that the payments made are in conformity with the National Insurance and Social Security Regulations.
|
The total remittances for the year to date is $ ________________________ |
|
||
10. |
The schedule of employees consists of |
________________________ pages. |
||
|
|
11. |
Signature of Employer: |
__________________ |
|
|
|
(or Representative) |
|
|
|
12. |
Date: |
__________________ |
|
|
13. |
Employer’s Stamp: |
__________________ |
FORM: CS3
R & P Dept (Revised March. 2006)