

You may prepare Form Dc 263 effectively by using our PDFinity® editor. FormsPal development team is always endeavoring to develop the tool and help it become even easier for users with its handy features. Unlock an constantly innovative experience now - take a look at and uncover new opportunities along the way! Getting underway is easy! All you should do is stick to the following simple steps directly below:
Step 1: Click on the "Get Form" button above. It'll open our pdf tool so you can start filling out your form.
Step 2: When you access the tool, there'll be the document prepared to be filled in. Other than filling in various fields, you can also do some other things with the Document, such as adding custom words, changing the initial text, inserting images, affixing your signature to the document, and much more.
Be attentive while completing this pdf. Ensure every blank is filled in accurately.
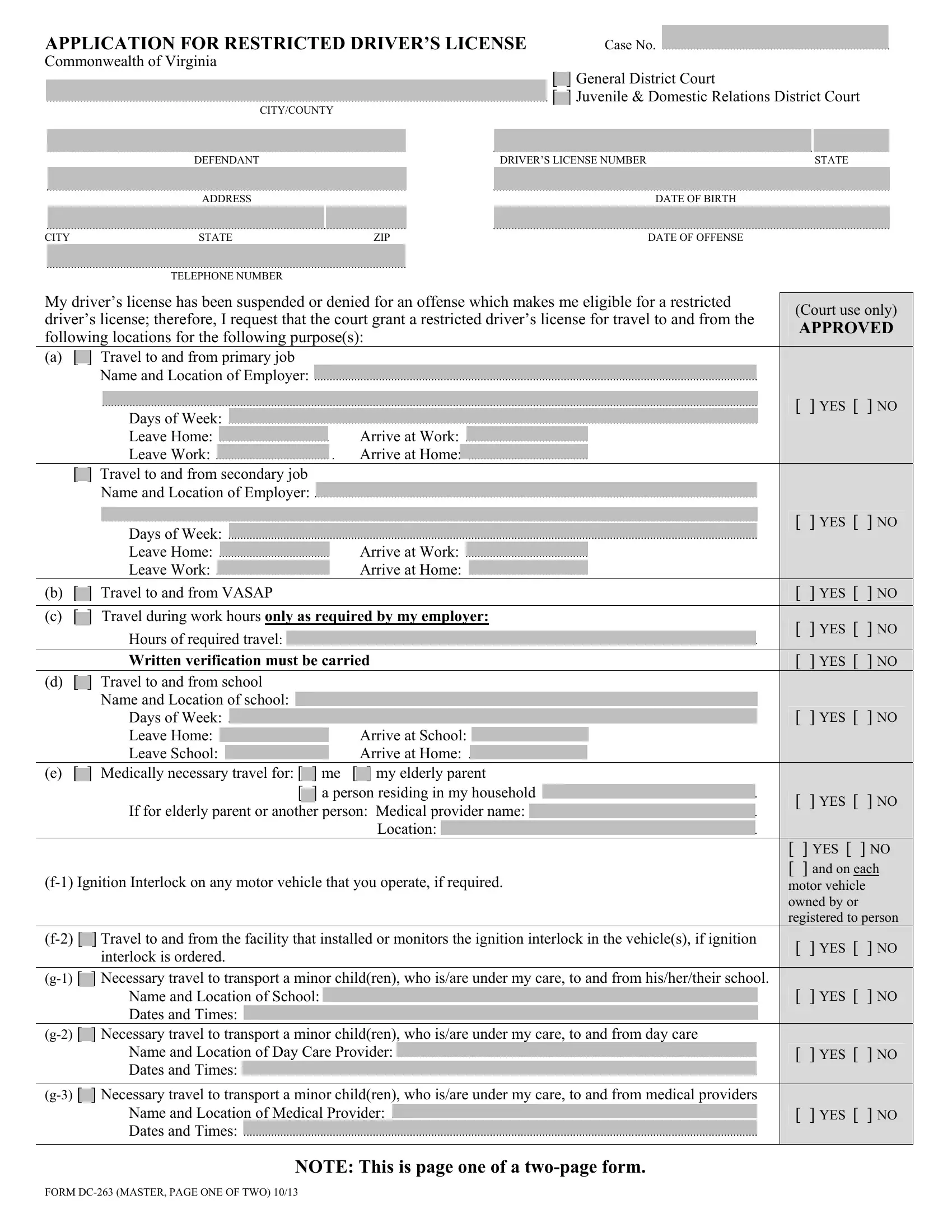
1. To start off, when filling out the Form Dc 263, start in the part that includes the following fields:
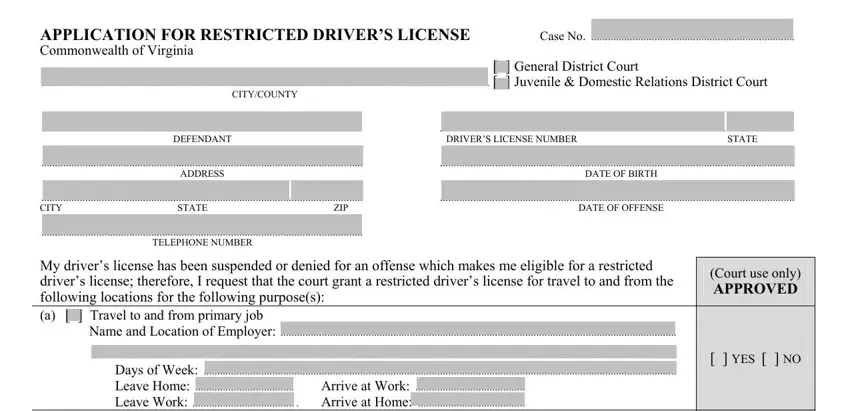
2. Soon after the last selection of blanks is done, go on to type in the applicable details in all these - Days of Week Leave Home Arrive, Travel to and from secondary job, Name and Location of Employer, Days of Week Leave Home Leave, Arrive at Work Arrive at Home, b Travel to and from VASAP c, Hours of required travel Written, d Travel to and from school, Name and Location of school Days, Arrive at School Arrive at Home, e Medically necessary travel for, f Ignition Interlock on any motor, YES NO, YES NO, and YES NO.
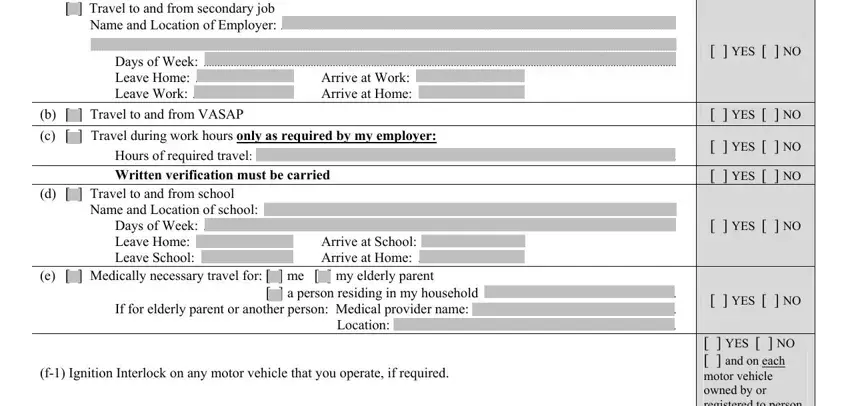
3. This subsequent step should also be fairly uncomplicated, f Travel to and from the, interlock is ordered, g Necessary travel to transport, Name and Location of School Dates, g Necessary travel to transport, Name and Location of Day Care, FORM DC MASTER PAGE ONE OF TWO, NOTE This is page one of a twopage, YES NO and on each motor, YES NO, YES NO, YES NO, and YES NO - all these blanks has to be filled out here.
4. The following section needs your attention in the following places: Name, Case No, h Necessary travel for Court, CONTINUED FROM PAGE, Names Location of Children Days, i Travel to and from, Name and Location of Probation, i Travel to and from programs, Program Name and Location Program, j Travel to and from a place of, Name and Location of place of, YES NO, YES NO, YES NO, and YES NO. It is important to enter all of the required information to move further.
It's very easy to make errors when filling in the YES NO, for that reason ensure that you look again before you decide to send it in.
5. This last stage to conclude this form is pivotal. Make certain you fill in the mandatory blank fields, consisting of m Travel to and from jail to, YES NO, I certify that the above, DATE, Reviewed and Approved as, DATE, DEFENDANTS SIGNATURE, and JUDGE, prior to using the pdf. Otherwise, it can give you an unfinished and possibly nonvalid form!
Step 3: Prior to moving forward, check that blank fields have been filled out the right way. The moment you believe it's all fine, click “Done." Obtain the Form Dc 263 the instant you subscribe to a free trial. Easily get access to the form inside your FormsPal cabinet, along with any modifications and changes being conveniently saved! FormsPal provides protected form completion with no data record-keeping or any sort of sharing. Be assured that your information is in good hands with us!