

Form De 2523 can be completed easily. Simply make use of FormsPal PDF editing tool to accomplish the job quickly. Our tool is continually evolving to give the best user experience possible, and that's due to our dedication to continuous enhancement and listening closely to customer opinions. Here's what you'd need to do to start:
Step 1: Firstly, open the pdf tool by pressing the "Get Form Button" above on this webpage.
Step 2: With the help of this handy PDF tool, you can actually do more than simply complete blank fields. Edit away and make your docs appear faultless with customized textual content put in, or modify the file's original input to perfection - all that comes with an ability to add any graphics and sign the PDF off.
When it comes to fields of this specific PDF, this is what you need to know:
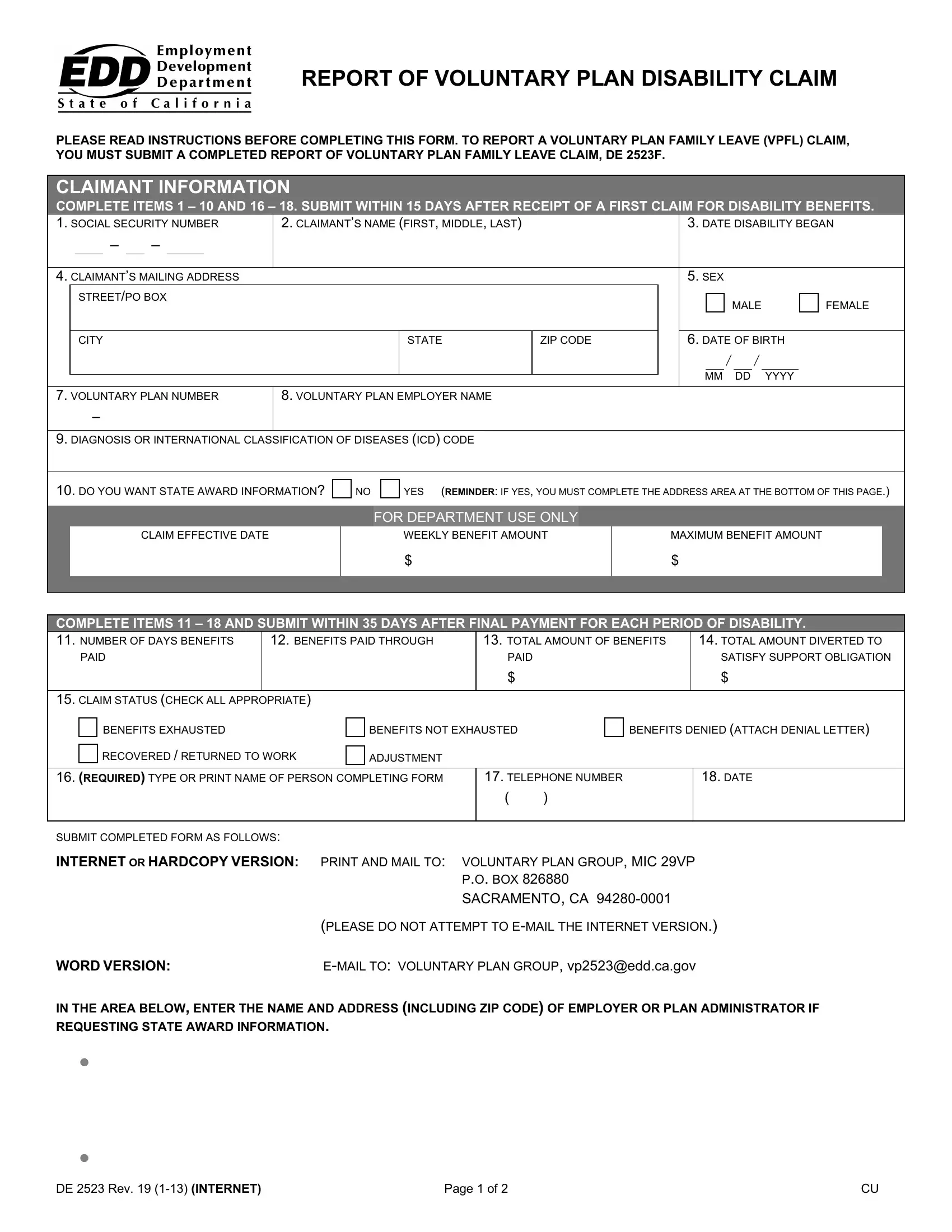
1. To start with, while filling out the Form De 2523, begin with the page that has the subsequent blank fields:
2. The subsequent stage is usually to fill in these particular fields: COMPLETE ITEMS AND SUBMIT, TOTAL AMOUNT OF BENEFITS, BENEFITS PAID THROUGH, TOTAL AMOUNT DIVERTED TO, PAID, CLAIM STATUS CHECK ALL APPROPRIATE, PAID, SATISFY SUPPORT OBLIGATION, BENEFITS EXHAUSTED, BENEFITS NOT EXHAUSTED, BENEFITS DENIED ATTACH DENIAL, RECOVERED RETURNED TO WORK, ADJUSTMENT, REQUIRED TYPE OR PRINT NAME OF, and TELEPHONE NUMBER.
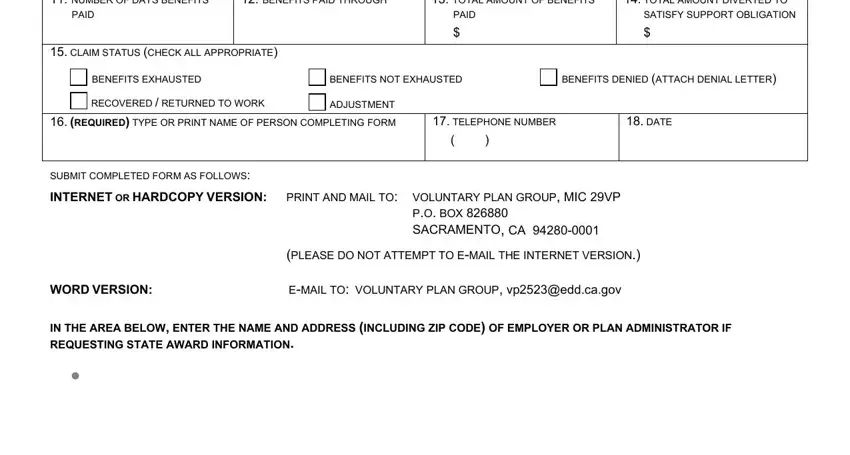
3. The third step is usually straightforward - fill out all the blanks in PRINT and MAIL TO, EMAIL TO, Voluntary Plan Group MIC VP PO Box, Please do not attempt to email the, Voluntary Plan Group vpeddcagov, You may also print and mail your, Voluntary Plan Group MIC VP PO Box, DE Rev INTERNET, and Page of to conclude this process.
Be extremely careful when filling out DE Rev INTERNET and You may also print and mail your, since this is where a lot of people make a few mistakes.
Step 3: Be certain that the information is correct and then just click "Done" to conclude the task. Try a free trial plan with us and obtain instant access to Form De 2523 - with all transformations saved and accessible inside your personal cabinet. When using FormsPal, you're able to complete documents without the need to be concerned about personal data breaches or entries getting distributed. Our protected software makes sure that your private data is stored safe.