
With the help of the online PDF tool by FormsPal, you'll be able to fill out or modify MRMIP here. In order to make our editor better and easier to use, we consistently come up with new features, with our users' suggestions in mind. In case you are looking to get going, this is what you will need to do:
Step 1: Hit the "Get Form" button above on this page to open our editor.
Step 2: With our handy PDF editing tool, you may do more than just fill out blank fields. Express yourself and make your documents seem great with customized textual content incorporated, or modify the original input to perfection - all that comes with an ability to incorporate your own pictures and sign the file off.
It will be straightforward to complete the form using out helpful tutorial! This is what you have to do:
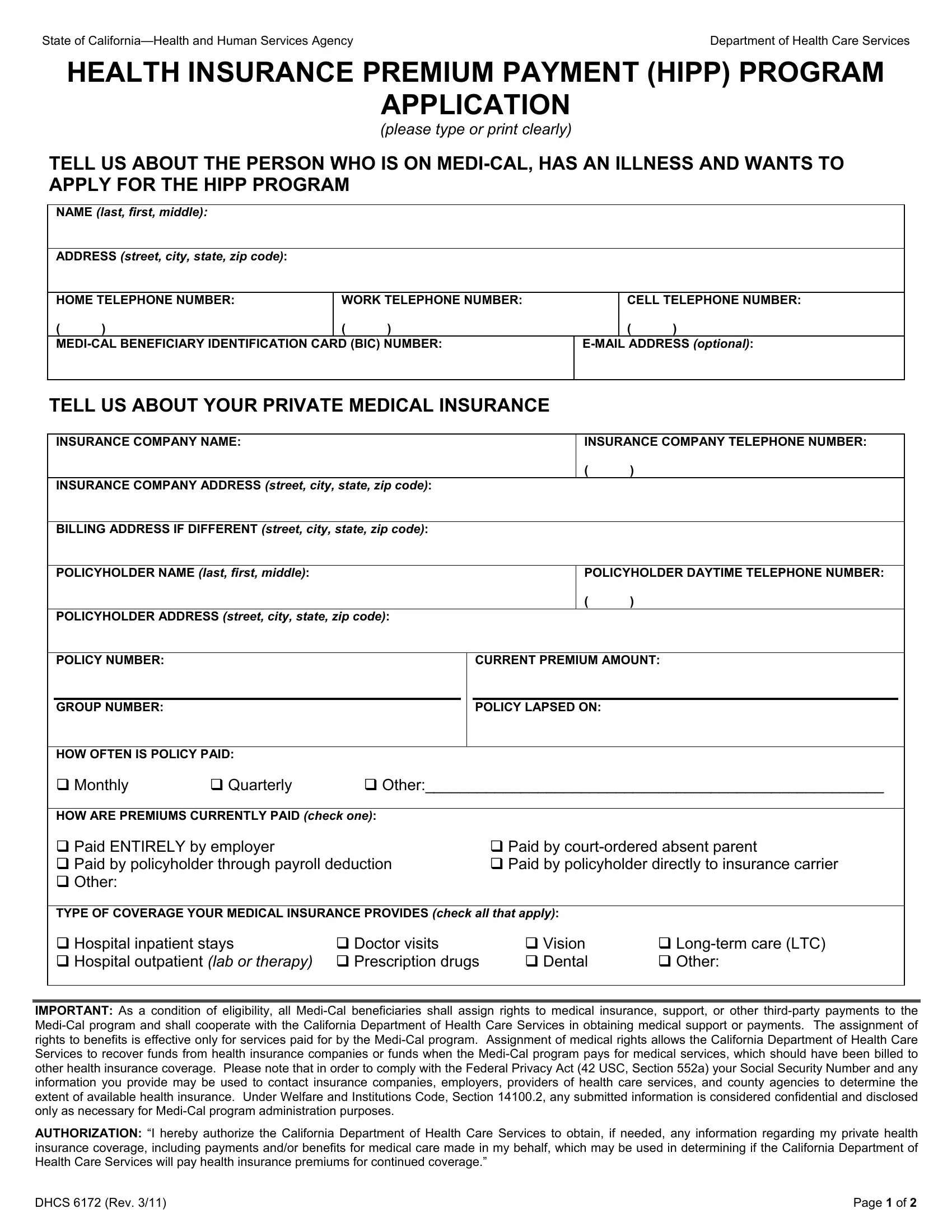
1. When filling out the MRMIP, make sure to include all of the important blank fields within the associated part. This will help to expedite the work, making it possible for your information to be processed quickly and appropriately.
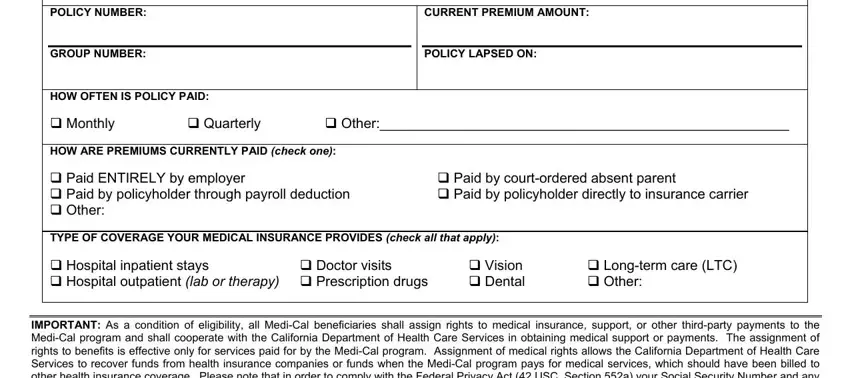
2. After this part is filled out, proceed to type in the applicable information in these - POLICYHOLDER ADDRESS street city, HOW OFTEN IS POLICY PAID Monthly, Doctor visits, Quarterly, Other, CURRENT PREMIUM AMOUNT, POLICY LAPSED ON, Paid by courtordered absent, Vision Dental, Longterm care LTC Other, and IMPORTANT As a condition of.
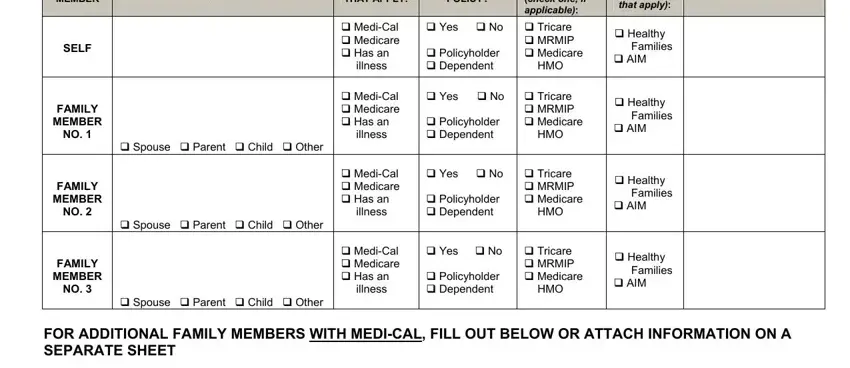
3. In this part, take a look at NAME last first middle, CHECK ALL THAT APPLY, POLICY, check one if applicable Tricare, Yes No Policyholder Dependent, Yes No Policyholder Dependent, Tricare MRMIP Medicare, HMO, MediCal Medicare Has an illness, MediCal Medicare Has an illness, MediCal Medicare Has an illness, Yes No Policyholder Dependent, Tricare MRMIP Medicare, HMO, and Healthy AIM. Each one of these need to be filled out with utmost attention to detail.
4. Your next paragraph needs your input in the following areas: Declaration I declare under, Name of Applicant print, Signature of ApplicantGuardian, Name of Policyholder print, Signature of Policyholder, Date, and Date. Be sure to enter all required details to move forward.
Concerning Date and Signature of ApplicantGuardian, be certain you don't make any errors here. These two are considered the most important ones in this file.
Step 3: Revise all the information you have typed into the blanks and then click the "Done" button. Make a free trial subscription with us and get direct access to MRMIP - download, email, or edit inside your FormsPal cabinet. Here at FormsPal, we do our utmost to be sure that all of your details are stored protected.