If you are a U.S. citizen or permanent resident and want to bring your spouse or child to live with you in the United States, you may be able to file Form I-730, Refugee/Asylee Relative Petition. This form is used to apply for refugee/asylee relative status for your spouse or child. There are certain requirements that must be met in order to file this form. To find out if you are eligible, please read on. Form Dhs 1144B allows for a foreign national who has been admitted as a bona fide refugee pursuant 8 CFR Section 207.3 and who is residing in the United States with his or her refugee-petitioning U.S.-citizen spouse or parent to apply for classification as an accompanying refugee relative . The entire application process from start to finish will take about eighteen (18) months and once approved the beneficiary will receive a conditional green card valid for two years .The interview process usually takes place at the nearest USCIS Regional Service Center where the initial applicat
| Question | Answer |
|---|---|
| Form Name | Form Dhs 1144B |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | DHS 1144B does california have medquest in sacramento form |
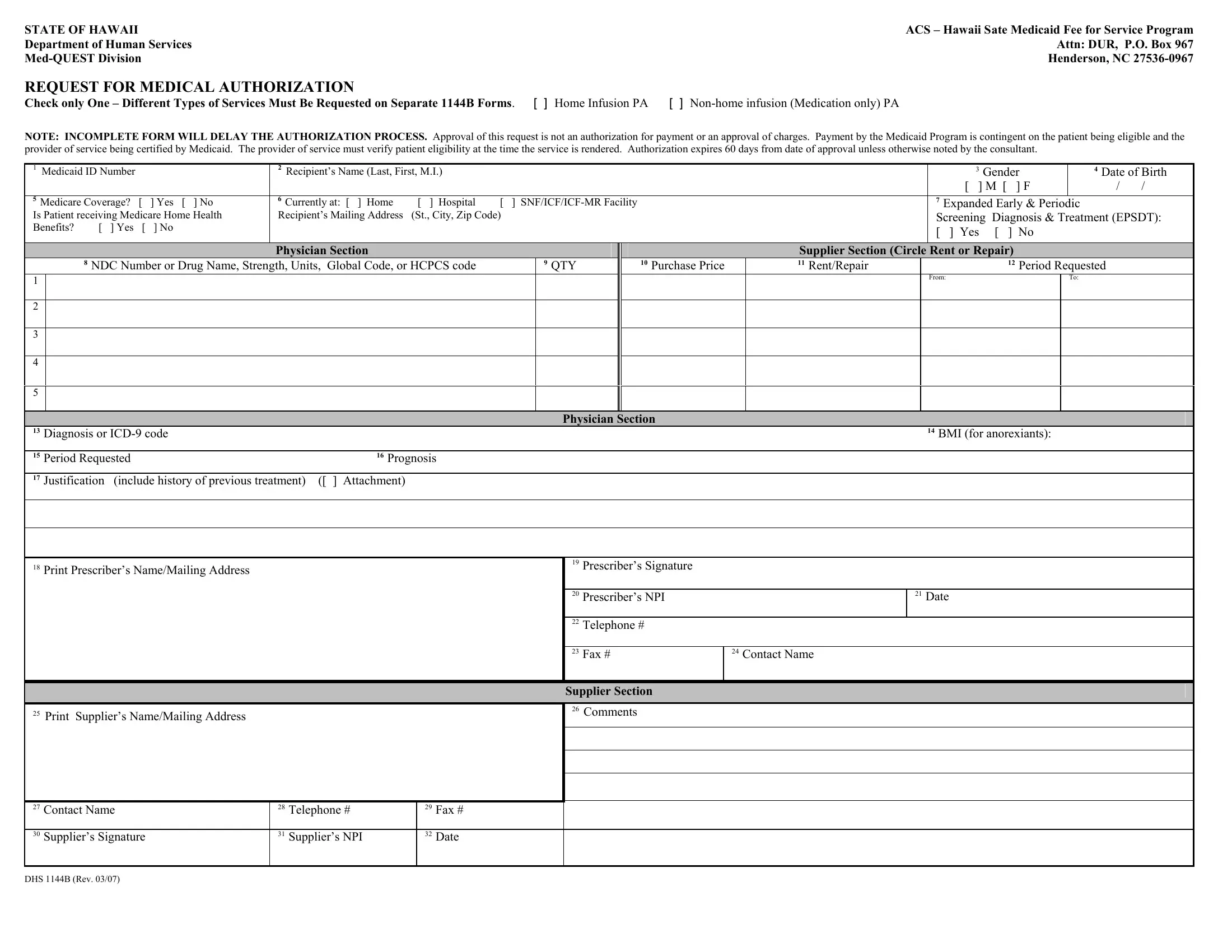
STATE OF HAWAII
Department of Human Services
ACS – Hawaii Sate Medicaid Fee for Service Program Attn: DUR, P.O. Box 967 Henderson, NC
REQUEST FOR MEDICAL AUTHORIZATION
Check only One – Different Types of Services Must Be Requested on Separate 1144B Forms. [ ] Home Infusion PA [ ]
NOTE: INCOMPLETE FORM WILL DELAY THE AUTHORIZATION PROCESS. Approval of this request is not an authorization for payment or an approval of charges. Payment by the Medicaid Program is contingent on the patient being eligible and the provider of service being certified by Medicaid. The provider of service must verify patient eligibility at the time the service is rendered. Authorization expires 60 days from date of approval unless otherwise noted by the consultant.
1 Medicaid ID Number |
|
|
2 Recipient’s Name (Last, First, M.I.) |
|
|
|
|
|
|
|
3 Gender |
|
4 Date of Birth |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
[ ] M [ |
] F |
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
5 Medicare Coverage? |
[ |
] Yes [ ] No |
6 Currently at: [ ] Home |
[ ] Hospital |
[ |
] |
|
|
|
7 Expanded Early & Periodic |
|
|
|||||||
Is Patient receiving Medicare Home Health |
Recipient’s Mailing Address |
(St., City, Zip Code) |
|
|
|
|
|
|
Screening Diagnosis & Treatment (EPSDT): |
||||||||||
Benefits? |
[ ] Yes |
[ |
] No |
|
|
|
|
|
|
|
|
|
[ ] Yes [ |
] No |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
Physician Section |
|
|
|
|
|
|
Supplier Section (Circle Rent or Repair) |
|
|
|||||
|
|
8 NDC Number or Drug Name, Strength, Units, Global Code, or HCPCS code |
|
|
9 QTY |
|
10 Purchase Price |
11 Rent/Repair |
|
12 Period Requested |
|
||||||||
1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
From: |
|
|
To: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Physician Section |
|
|
|
|
|
|
|
|
||
13 Diagnosis or |
|
|
|
|
|
|
|
|
|
14 BMI (for anorexiants): |
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
15 Period Requested |
|
|
16 Prognosis |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
17 Justification (include history of previous treatment) ([ ] Attachment) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
18Print Prescriber’s Name/Mailing Address
19Prescriber’s Signature
20 Prescriber’s NPI |
21 Date |
|
|
22Telephone #
23 Fax # |
24 Contact Name |
|
|
25 Print Supplier’s Name/Mailing Address
Supplier Section
26Comments
27 |
Contact Name |
28 |
Telephone # |
29 |
Fax # |
|
|
|
|
|
|
|
|
30 |
Supplier’s Signature |
31 |
Supplier’s NPI |
32 |
Date |
|
|
|
|
|
|
|
|
DHS 1144B (Rev. 03/07)