On November 11, 1918, the armistice was signed between the Allies and Germany, ending World War I. This document, referred to as Form DHS 1918, is a form that was used to formally declare the end of hostilities. The document is now held in the National Archives in London. This form is an important piece of history, as it represents the formal end of World War I. It is also interesting from a legal standpoint, as it provides insight into the process that was followed to officially end the war. The National Archives has created a digital version of this form that can be viewed online.
| Question | Answer |
|---|---|
| Form Name | Form Dhs 1918 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | FIA1918_10573_7 change in central registry clearance request michigan dhs form |
For Office Use Only
Birth Date
Adoptee’s Birth Name (Last, First, Middle)
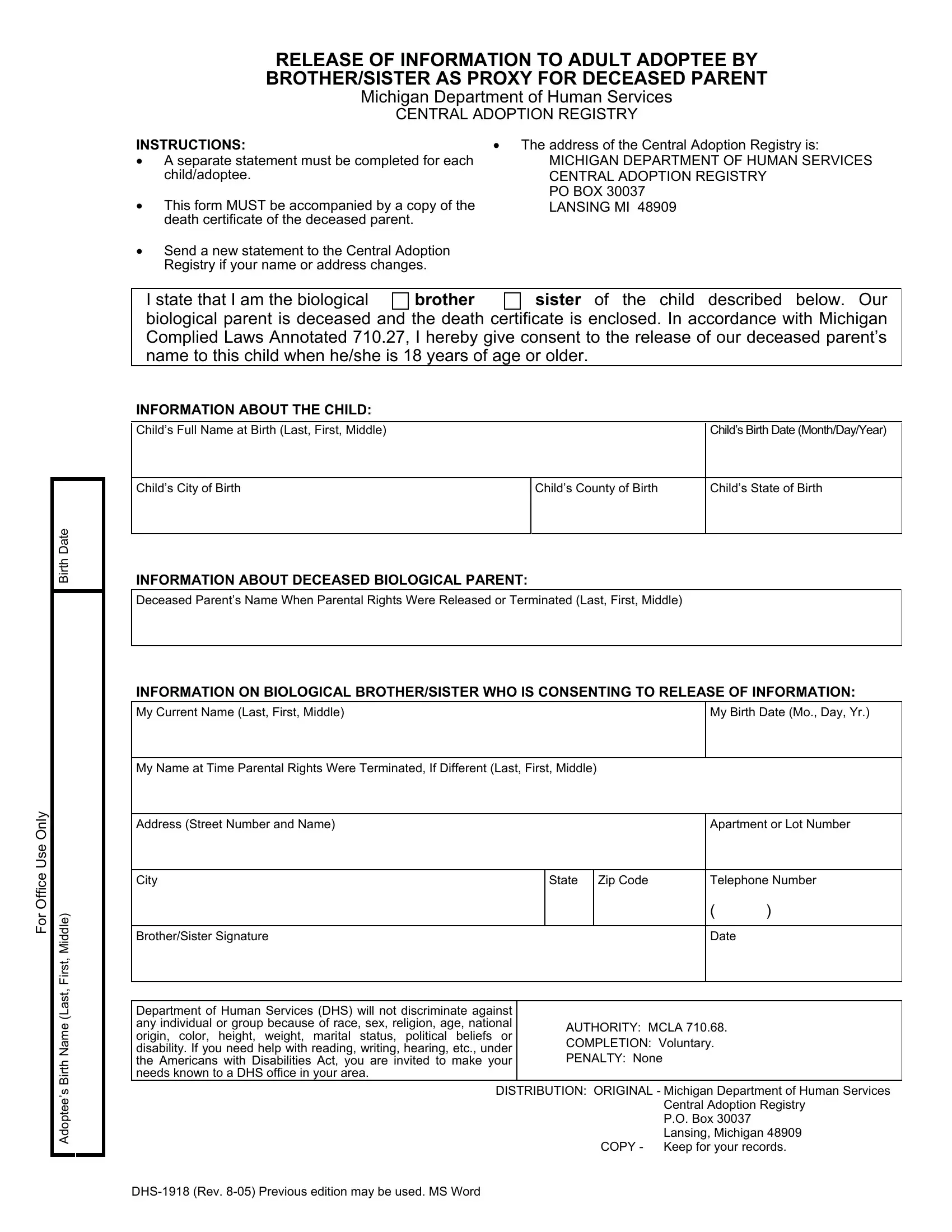
RELEASE OF INFORMATION TO ADULT ADOPTEE BY
BROTHER/SISTER AS PROXY FOR DECEASED PARENT
Michigan Department of Human Services
CENTRAL ADOPTION REGISTRY
INSTRUCTIONS: |
|
• The address of the Central Adoption Registry is: |
• A separate statement must be completed for each |
MICHIGAN DEPARTMENT OF HUMAN SERVICES |
|
child/adoptee. |
|
CENTRAL ADOPTION REGISTRY |
• This form MUST be accompanied by a copy of the |
PO BOX 30037 |
|
LANSING MI 48909 |
||
death certificate of the deceased parent. |
|
|
• Send a new statement to the Central Adoption |
|
|
Registry if your name or address changes. |
|
|
|
|
|
I state that I am the biological |
BROTHER |
SISTER of the child described below. Our |
biological parent is deceased and the death certificate is enclosed. In accordance with Michigan Complied Laws Annotated 710.27, I hereby give consent to the release of our deceased parent’s name to this child when he/she is 18 years of age or older.
INFORMATION ABOUT THE CHILD:
Child’s Full Name at Birth (Last, First, Middle) |
|
Child’s Birth Date (Month/Day/Year) |
|
|
|
|
|
|
Child’s City of Birth |
Child’s County of Birth |
Child’s State of Birth |
|
|
|
INFORMATION ABOUT DECEASED BIOLOGICAL PARENT:
Deceased Parent’s Name When Parental Rights Were Released or Terminated (Last, First, Middle)
INFORMATION ON BIOLOGICAL BROTHER/SISTER WHO IS CONSENTING TO RELEASE OF INFORMATION:
My Current Name (Last, First, Middle) |
My Birth Date (Mo., Day, Yr.) |
|
|
My Name at Time Parental Rights Were Terminated, If Different (Last, First, Middle)
Address (Street Number and Name) |
|
|
|
Apartment or Lot Number |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
State |
Zip Code |
|
Telephone Number |
||
|
|
|
|
|
( |
) |
|
|
|
|
|
|
|
Brother/Sister Signature |
|
|
|
Date |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Department of Human Services (DHS) will not discriminate against |
|
|
|
|
|
|
any individual or group because of race, sex, religion, age, national |
|
AUTHORITY: MCLA 710.68. |
|
|||
origin, color, height, weight, marital status, political beliefs or |
|
|
||||
|
COMPLETION: Voluntary. |
|
||||
disability. If you need help with reading, writing, hearing, etc., under |
|
|
||||
|
PENALTY: None |
|
|
|
||
the Americans with Disabilities Act, you are invited to make your |
|
|
|
|
||
needs known to a DHS office in your area. |
|
|
|
|
|
|
DISTRIBUTION: ORIGINAL - Michigan Department of Human Services |
||||||
|
|
|
|
Central Adoption Registry |
||
|
|
|
|
P.O. Box 30037 |
|
|
|
|
|
|
Lansing, Michigan 48909 |
||
|
|
|
COPY - Keep for your records. |
|||
|
|
|
|
|
||