Form Doh 30 is a document that some businesses are required to file in order to notify the state of their intention to raise money through an equity or debt offering. This document can be complex, and businesses should seek legal assistance in completing it. In this blog post, we will discuss what Form Doh 30 is, who needs to file it, and the consequences of not filing it. We also provide a link to a more detailed explanation of Form Doh 30 on the Pennsylvania Secretary of State's website.
| Question | Answer |
|---|---|
| Form Name | Form Doh 30 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | wdh30m adoption information registry new york 800 |
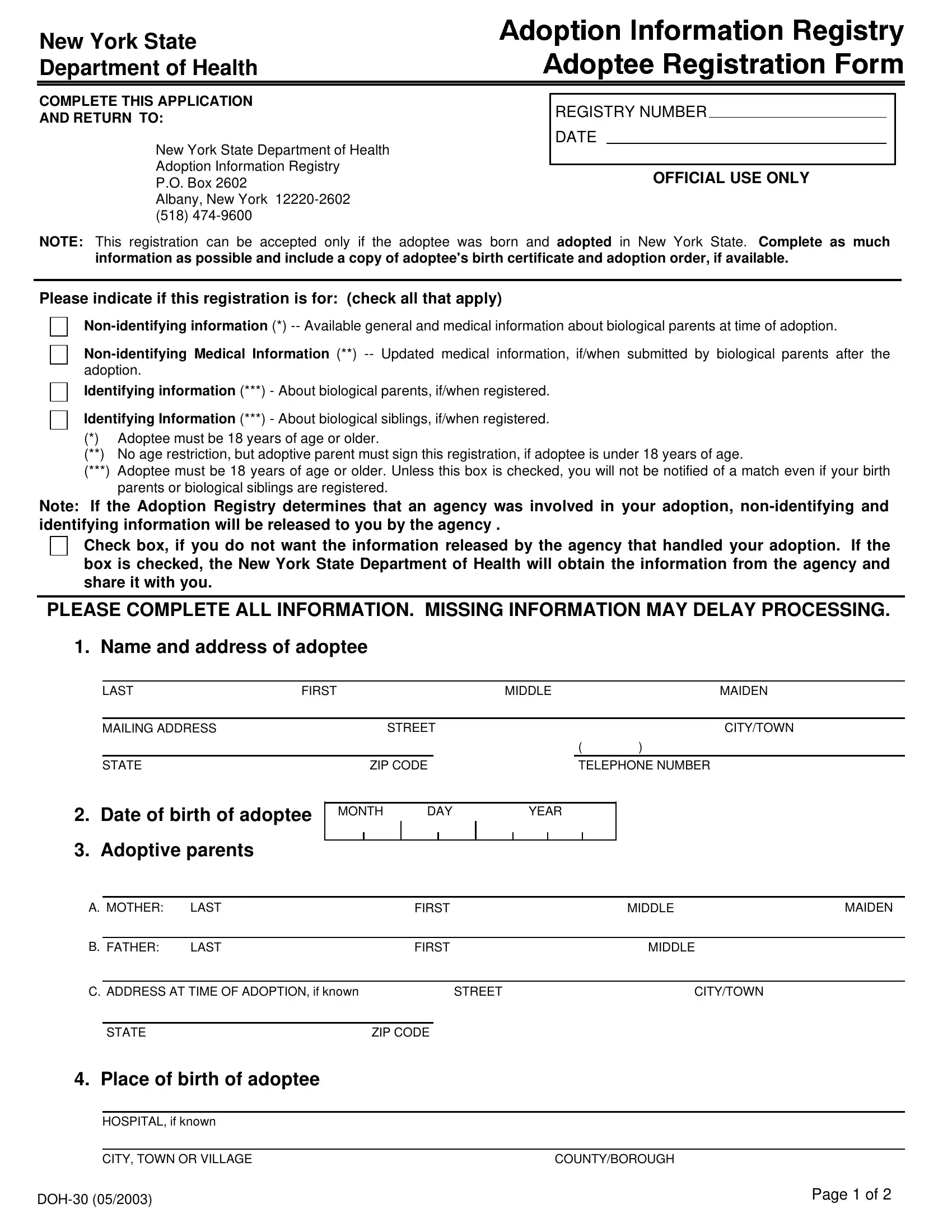
New York State Department of Health
COMPLETE THIS APPLICATION
AND RETURN TO:
New York State Department of Health Adoption Information Registry
P.O. Box 2602
Albany, New York
REGISTRY NUMBER
DATE
OFFICIAL USE ONLY
NOTE: This registration can be accepted only if the adoptee was born and adopted in New York State. Complete as much information as possible and include a copy of adoptee's birth certificate and adoption order, if available.
Please indicate if this registration is for: (check all that apply)
Identifying information (***) - About biological parents, if/when registered.
Identifying Information (***) - About biological siblings, if/when registered.
(*)Adoptee must be 18 years of age or older.
(**) No age restriction, but adoptive parent must sign this registration, if adoptee is under 18 years of age.
(***)Adoptee must be 18 years of age or older. Unless this box is checked, you will not be notified of a match even if your birth parents or biological siblings are registered.
Note: If the Adoption Registry determines that an agency was involved in your adoption,
Check box, if you do not want the information released by the agency that handled your adoption. If the box is checked, the New York State Department of Health will obtain the information from the agency and share it with you.
PLEASE COMPLETE ALL INFORMATION. MISSING INFORMATION MAY DELAY PROCESSING. 1. Name and address of adoptee
LAST |
FIRST |
|
MIDDLE |
MAIDEN |
|
|
|
|
|
|
|
MAILING ADDRESS |
|
STREET |
CITY/TOWN |
||
|
|
|
|
( |
) |
STATE
2.Date of birth of adoptee
3.Adoptive parents
|
ZIP CODE |
|
|
TELEPHONE NUMBER |
||||
|
|
|
|
|
|
|
|
|
MONTH |
DAY |
|
YEAR |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A. MOTHER: |
LAST |
FIRST |
MIDDLE |
MAIDEN |
||
|
|
|
|
|
|
|
B. FATHER: |
LAST |
FIRST |
MIDDLE |
|
||
|
|
|
|
|
|
|
C. ADDRESS AT TIME OF ADOPTION, if known |
|
STREET |
CITY/TOWN |
|
||
|
|
|
|
|
|
|
|
STATE |
|
ZIP CODE |
|
|
|
4. Place of birth of adoptee
HOSPITAL, if known
CITY, TOWN OR VILLAGE |
COUNTY/BOROUGH |
Page 1 of 2 |
|
|
5.Indicate the name of the agency and court of adoption, if known
A.NAME OF AGENCY
CITY, TOWN OR VILLAGE |
COUNTY/BOROUGH |
Check box if you have already received
Date received:
MONTH |
DAY |
YEAR |
|
|
|
MONTH |
DAY |
YEAR |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C. DATE OF ADOPTION |
|
|
|
||||
B. NAME OF COURT |
|
|
|
|
||||||
6. Is the adoptee in contact with birth brother(s) and/or sister(s)?
YES
NO If yes, please provide the following information for each sibling with whom adoptee is in contact.
NAME
DATE OF BIRTH
ADDRESS (include zip code)
1.
2.
3.
4.
5.
6.
7.
7. Signature and Notarization. |
heg |
State of
County of
SS.
I solemnly attest that all of the information provided on this application is true and accurate to the best of my knowledge under the penalty of perjury.
SIGNATURE OF REGISTRANT
Signature must be notarized
NOTE: Adoptive Parent must sign if the adoptee is under 18 years of age. Notarization must include Notary's stamp or raised seal.
Sworn to before me this |
|
|
Day |
||||
|
|
|
|
|
|
|
|
Of |
, |
. |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Notary Public |
|
|
|
|
|
|
|
|
|
|
Page 2 of 2 |
|||