


You are able to prepare Form-214 without difficulty with our PDF editor online. Our editor is constantly evolving to give the very best user experience attainable, and that is because of our commitment to continual enhancement and listening closely to customer comments. It just takes a few basic steps:
Step 1: Open the PDF file inside our tool by clicking the "Get Form Button" above on this webpage.
Step 2: With the help of this online PDF file editor, you can accomplish more than merely fill out blanks. Edit away and make your docs seem professional with custom text put in, or adjust the original input to excellence - all that comes along with an ability to add any type of pictures and sign the PDF off.
Filling out this document demands care for details. Ensure that every blank field is done correctly.
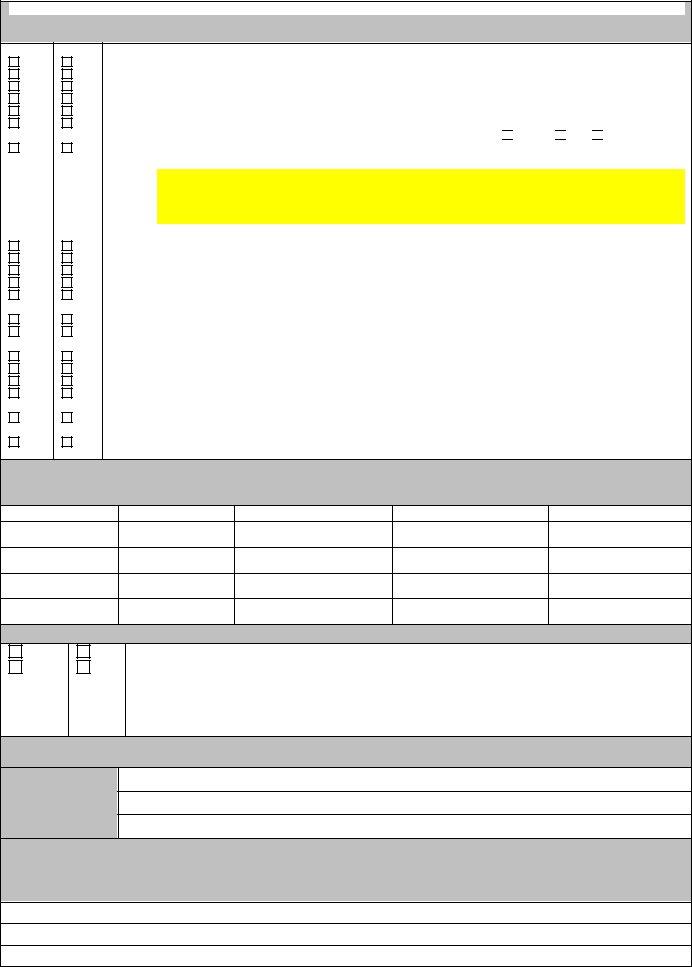
1. First of all, once completing the Form-214, start out with the part that features the following blanks:
2. Given that the last segment is complete, you need to add the needed specifics in Previous residences Complete this, ADDRESS, CITY, STATE, FROM, DATES, NAME OF COMPANYBUSINESSFIRM ETC, ADDRESS, PLACE OF, EMPLOYMENT, CITY, STATE, POSTAL CODE, NAME OF SUPERVISOR, and CONTACT NUMBER allowing you to move forward to the third step.
3. The third stage is normally simple - fill out all of the blanks in YES YES YES YES YES YES, YES, YES YES YES YES YES, YES YES, YES YES YES YES, YES, NO NO NO NO NO NO, NO NO NO NO NO, NO NO, NO NO NO NO, YES, Are you a United States Citizen, You MUST indicate the type of, Both, and Have you ever been arrested for to complete this segment.
4. It's time to start working on this fourth segment! Here you will get these Date of Arrest, Charge, Location CityState, Disposition, Arresting Agency, MILITARY SERVICE, YES YES, NO NO, Have you ever served in the Armed, If actively serving in the Armed, If you answered Yes to questions, MEDICAL INFORMATION, Treating Physician, Name, and Address fields to do.
5. Since you near the end of this document, you'll find several extra things to complete. Mainly, STATE OF LOUISIANA PARISH OF, Affiants Name Printed, Affiants Address Printed, and I having been duly sworn depose must be done.
Be very careful when filling out Affiants Address Printed and I having been duly sworn depose, as this is the section where many people make a few mistakes.
Step 3: Once you have glanced through the information in the file's blanks, click on "Done" to conclude your form at FormsPal. Join FormsPal right now and immediately get access to Form-214, available for download. All modifications made by you are kept , which enables you to change the form at a later point if required. When you use FormsPal, you can certainly fill out forms without the need to be concerned about information incidents or records being distributed. Our protected platform makes sure that your personal data is stored safely.