The Department of Social and Health Services (DSHS) is responsible for administering a number of assistance programs in Washington State, including Temporary Assistance for Needy Families (TANF), which provides cash assistance to low-income families. If you're currently receiving TANF benefits, it's important to understand the rules and regulations governing your benefits, including how and when you can receive payments. In this blog post, we'll provide an overview of the DSHS 13 633 form, which outlines the payment schedules and eligibility requirements for TANF recipients in Washington State. Stay tuned for future posts with more information on TANF benefits!
| Question | Answer |
|---|---|
| Form Name | Form Dshs 13 633 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | 18_633 dshs ein number form |
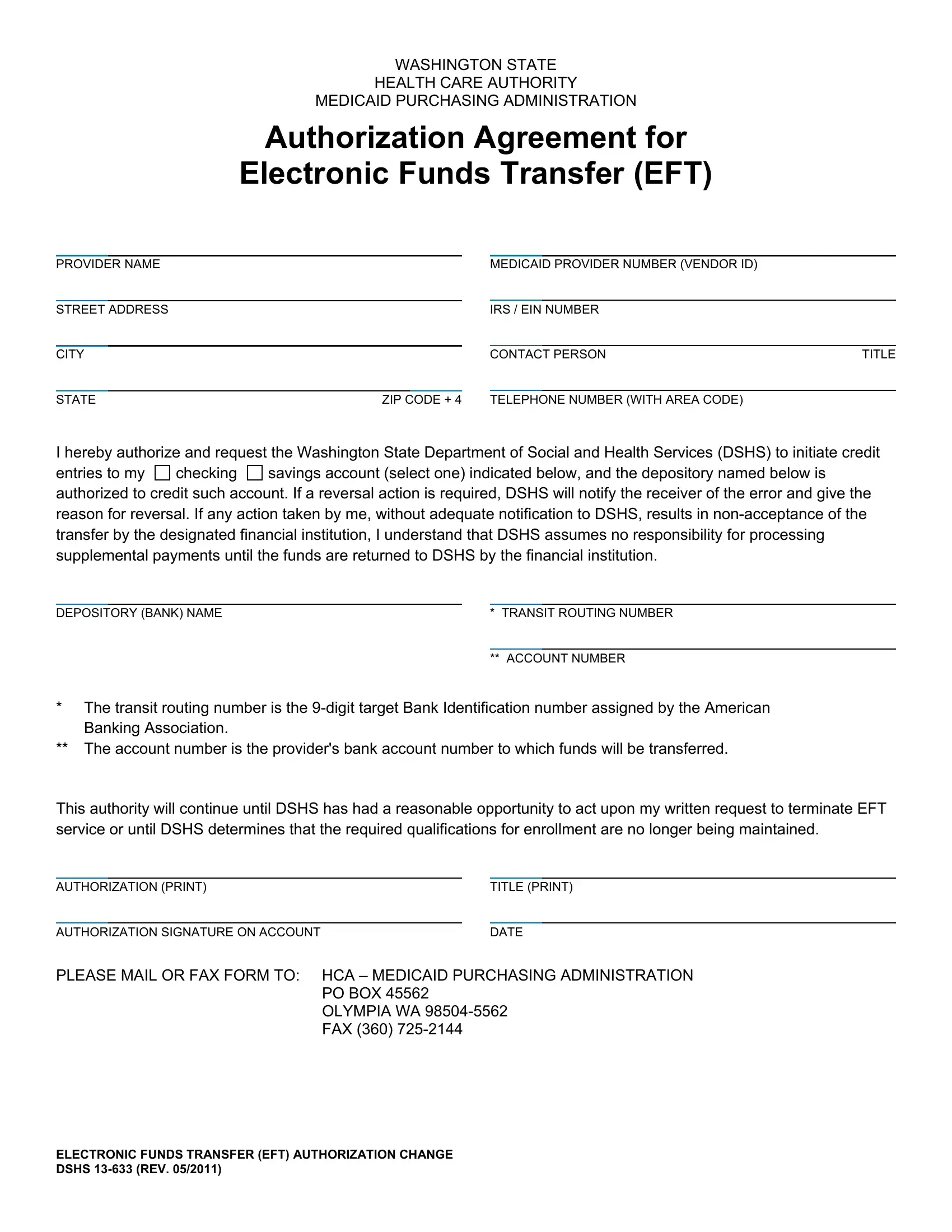
WASHINGTON STATE
HEALTH CARE AUTHORITY
MEDICAID PURCHASING ADMINISTRATION
Authorization Agreement for
Electronic Funds Transfer (EFT)
PROVIDER NAME |
|
|
|
MEDICAID PROVIDER NUMBER (VENDOR ID) |
|
||
|
|
|
|
|
|
|
|
STREET ADDRESS |
|
|
IRS / EIN NUMBER |
|
|||
|
|
|
|
|
|
|
|
CITY |
|
|
CONTACT PERSON |
TITLE |
|||
|
|
|
|
|
|
|
|
STATE |
ZIP CODE + 4 |
|
TELEPHONE NUMBER (WITH AREA CODE) |
|
|||
I hereby authorize and request the Washington State Department of Social and Health Services (DSHS) to initiate credit entries to my checking savings account (select one) indicated below, and the depository named below is authorized to credit such account. If a reversal action is required, DSHS will notify the receiver of the error and give the reason for reversal. If any action taken by me, without adequate notification to DSHS, results in
DEPOSITORY (BANK) NAME |
* TRANSIT ROUTING NUMBER |
|
|
|
|
|
** ACCOUNT NUMBER |
|
*The transit routing number is the
**The account number is the provider's bank account number to which funds will be transferred.
This authority will continue until DSHS has had a reasonable opportunity to act upon my written request to terminate EFT service or until DSHS determines that the required qualifications for enrollment are no longer being maintained.
AUTHORIZATION (PRINT) |
|
TITLE (PRINT) |
||
|
|
|
|
|
AUTHORIZATION SIGNATURE ON ACCOUNT |
|
DATE |
||
PLEASE MAIL OR FAX FORM TO: HCA – MEDICAID PURCHASING ADMINISTRATION
PO BOX 45562 OLYMPIA WA
ELECTRONIC FUNDS TRANSFER (EFT) AUTHORIZATION CHANGE DSHS