
Handling PDF files online can be surprisingly easy using our PDF tool. You can fill out Form F 12022 here effortlessly. The editor is constantly updated by our staff, acquiring new awesome functions and growing to be a lot more convenient. Here's what you'll need to do to begin:
Step 1: Access the PDF in our tool by clicking on the "Get Form Button" at the top of this page.
Step 2: Once you launch the file editor, you will see the form all set to be completed. Apart from filling out different blank fields, you might also perform several other actions with the form, including putting on any words, modifying the original text, adding illustrations or photos, affixing your signature to the form, and a lot more.
This PDF form requires particular info to be typed in, thus you should definitely take the time to fill in exactly what is asked:
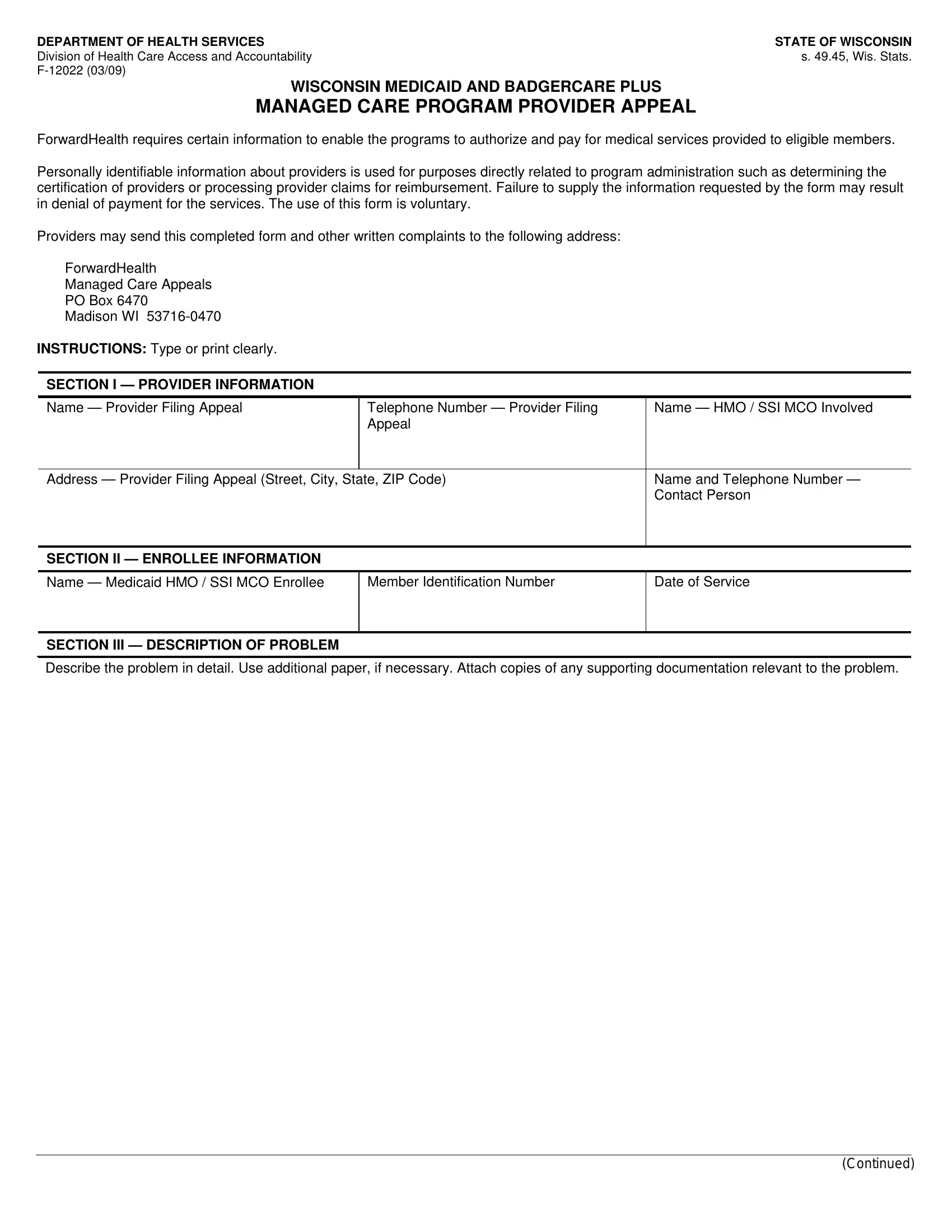
1. Whenever filling in the Form F 12022, make sure to incorporate all necessary fields in its associated section. It will help expedite the process, allowing for your details to be handled quickly and appropriately.
2. The next part would be to fill in the next few blanks: Insert date the appeal was sent to, Insert date the appeal, and What response was received from.
It's easy to get it wrong while filling out the What response was received from, and so be sure you look again before you decide to submit it.
3. The following section is about What does the provider consider to, SECTION IV SIGNATURE, This information is accurate to, SIGNATURE Provider, and Date Signed - fill out each of these fields.
Step 3: Reread all the details you've entered into the form fields and then click on the "Done" button. Sign up with us today and immediately obtain Form F 12022, prepared for download. Every modification made is conveniently saved , which means you can edit the pdf at a later point when necessary. When using FormsPal, you can certainly complete documents without stressing about personal information incidents or records getting shared. Our protected platform ensures that your personal details are stored safely.