
Form F 44151 can be completed with ease. Just use FormsPal PDF editing tool to complete the task fast. We at FormsPal are dedicated to making sure you have the ideal experience with our tool by constantly introducing new functions and improvements. With these improvements, using our editor becomes easier than ever! Getting underway is simple! Everything you should do is stick to the following simple steps directly below:
Step 1: First, open the editor by pressing the "Get Form Button" in the top section of this page.
Step 2: With the help of this state-of-the-art PDF tool, you are able to do more than just fill in forms. Try all of the features and make your docs look high-quality with custom textual content incorporated, or optimize the original content to excellence - all supported by an ability to incorporate your own graphics and sign it off.
As for the fields of this specific PDF, this is what you should consider:
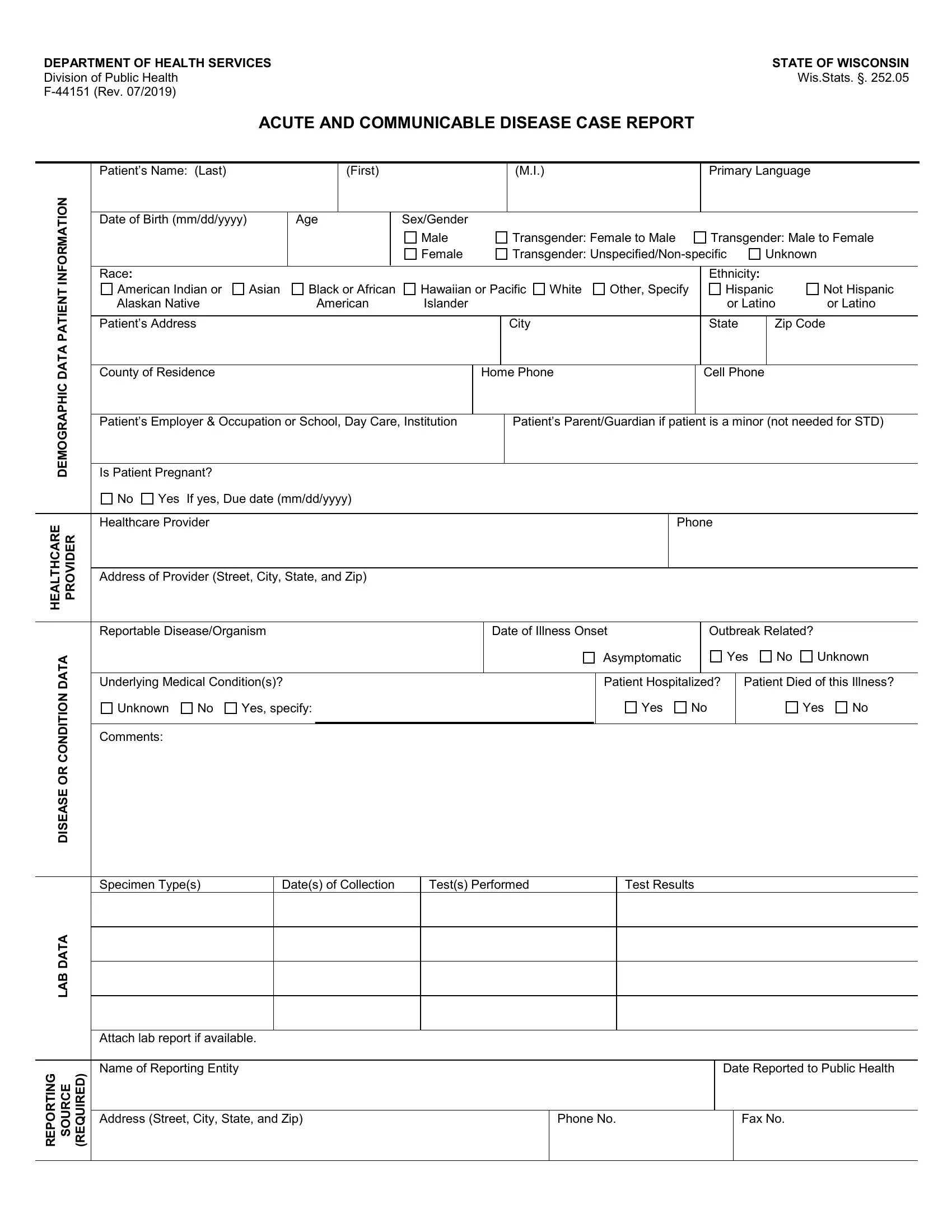
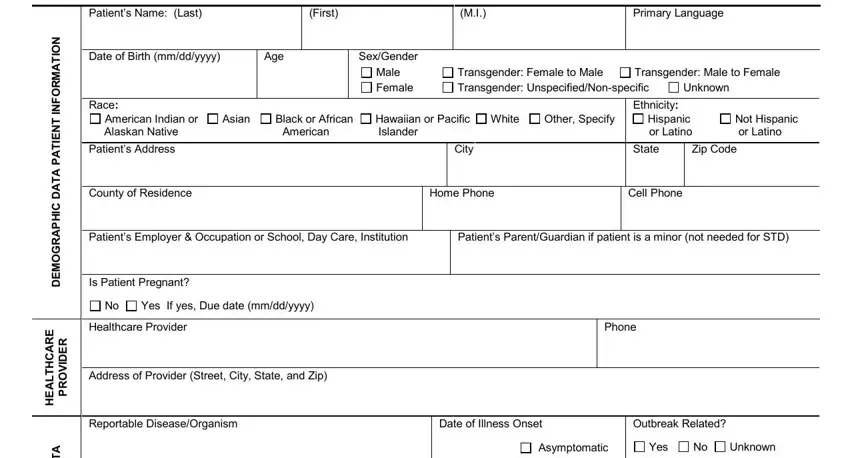
1. First of all, once filling out the Form F 44151, start with the form section that features the subsequent fields:
2. Now that this segment is done, it is time to insert the needed specifics in A T A D N O T D N O C R O E S A E, A T A D B A L, G N T R O P E R, E C R U O S, Underlying Medical Conditions, Unknown, Yes specify, Comments, Patient Hospitalized, Patient Died of this Illness, Yes, Yes, Specimen Types, Dates of Collection, and Tests Performed in order to move forward further.
Be extremely attentive when completing G N T R O P E R and Tests Performed, since this is where many people make mistakes.
Step 3: After you have reviewed the information in the blanks, press "Done" to complete your form. Sign up with FormsPal now and easily use Form F 44151, set for downloading. Every change made is conveniently saved , allowing you to modify the file further when required. When you use FormsPal, it is simple to complete forms without the need to be concerned about personal data incidents or records getting shared. Our protected software makes sure that your personal details are kept safe.