Form F 62224 is a tax form that United States citizens and residents use to report interest earned on a foreign bank account. The form must be filed by April 15th each year, and the deadline for filing is extended to June 15th if you file for an automatic six-month extension. In order to complete the form, you'll need to provide information about your foreign bank account, including the name of the bank, its address, and the account number. You'll also need to report any interest earned on the account during the year. Penalties may apply if you fail to file Form F 62224 or if you underreport your income from foreign accounts. Contact your tax advisor if you have any questions about completing this form.
| Question | Answer |
|---|---|
| Form Name | Form F 62224 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | F62224 wisconsin division of health notice of substantial change form |
DEPARTMENT OF HEALTH SERVICES |
STATE OF WISCONSIN |
|
Division of Quality Assurance |
42 |
CFR 483.75, Subpart D |
HFS |
129, Wis. Admin. Code |
|
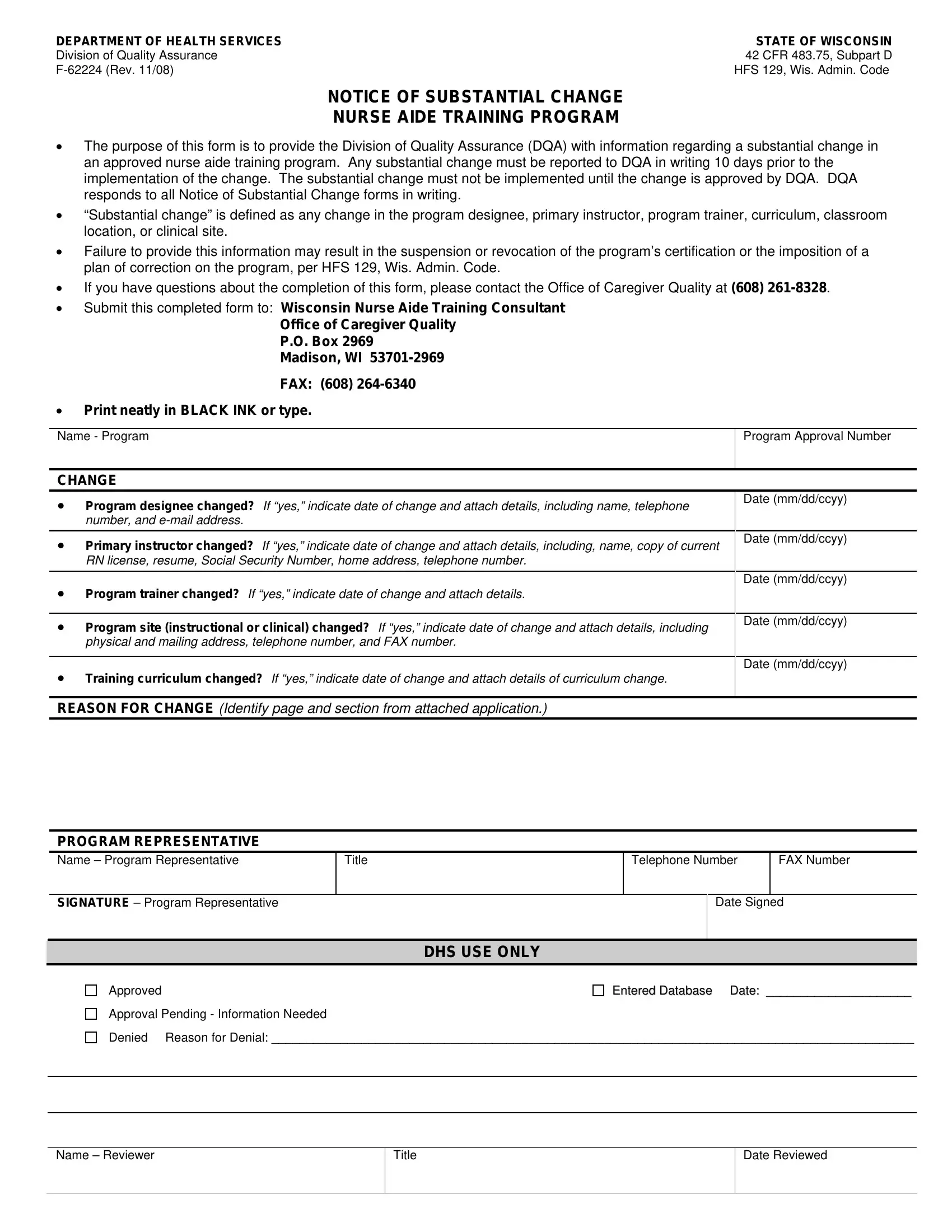
NOTICE OF SUBSTANTIAL CHANGE
NURSE AIDE TRAINING PROGRAM
•The purpose of this form is to provide the Division of Quality Assurance (DQA) with information regarding a substantial change in an approved nurse aide training program. Any substantial change must be reported to DQA in writing 10 days prior to the implementation of the change. The substantial change must not be implemented until the change is approved by DQA. DQA responds to all Notice of Substantial Change forms in writing.
•“Substantial change” is defined as any change in the program designee, primary instructor, program trainer, curriculum, classroom location, or clinical site.
•Failure to provide this information may result in the suspension or revocation of the program’s certification or the imposition of a plan of correction on the program, per HFS 129, Wis. Admin. Code.
•If you have questions about the completion of this form, please contact the Office of Caregiver Quality at (608)
•Submit this completed form to: Wisconsin Nurse Aide Training Consultant
Office of Caregiver Quality
P.O. Box 2969
Madison, WI
FAX: (608)
•Print neatly in BLACK INK or type.
Name - Program |
Program Approval Number |
|
|
CHANGE
• |
Program designee changed? If “yes,” indicate date of change and attach details, including name, telephone |
Date (mm/dd/ccyy) |
|
||
|
number, and |
|
|
|
|
• |
Primary instructor changed? If “yes,” indicate date of change and attach details, including, name, copy of current |
Date (mm/dd/ccyy) |
|
||
|
RN license, resume, Social Security Number, home address, telephone number. |
|
|
|
|
• |
|
Date (mm/dd/ccyy) |
Program trainer changed? If “yes,” indicate date of change and attach details. |
|
|
|
|
|
• |
Program site (instructional or clinical) changed? If “yes,” indicate date of change and attach details, including |
Date (mm/dd/ccyy) |
|
||
|
physical and mailing address, telephone number, and FAX number. |
|
|
|
|
• |
|
Date (mm/dd/ccyy) |
Training curriculum changed? If “yes,” indicate date of change and attach details of curriculum change. |
|
|
|
|
|
REASON FOR CHANGE (Identify page and section from attached application.)
PROGRAM REPRESENTATIVE
Name – Program Representative
Title
Telephone Number
FAX Number
SIGNATURE – Program Representative
Date Signed
|
DHS USE ONLY |
Approved |
Entered Database Date: _____________________ |
Approval Pending - Information Needed |
|
Denied |
Reason for Denial: _____________________________________________________________________________________________ |
|
|
|
|
Name – Reviewer
Title
Date Reviewed