
If you would like to fill out 675 approved omb, you don't have to install any kind of software - simply make use of our online tool. Our team is committed to providing you the perfect experience with our tool by constantly presenting new capabilities and upgrades. Our editor has become a lot more user-friendly with the most recent updates! At this point, editing PDF documents is simpler and faster than ever before. Here's what you'd want to do to get going:
Step 1: Simply hit the "Get Form Button" above on this page to access our pdf form editing tool. There you will find all that is needed to fill out your file.
Step 2: This tool grants the capability to modify PDF documents in a variety of ways. Change it by writing customized text, adjust what is originally in the document, and include a signature - all when you need it!
It really is an easy task to finish the document using out detailed tutorial! Here is what you should do:
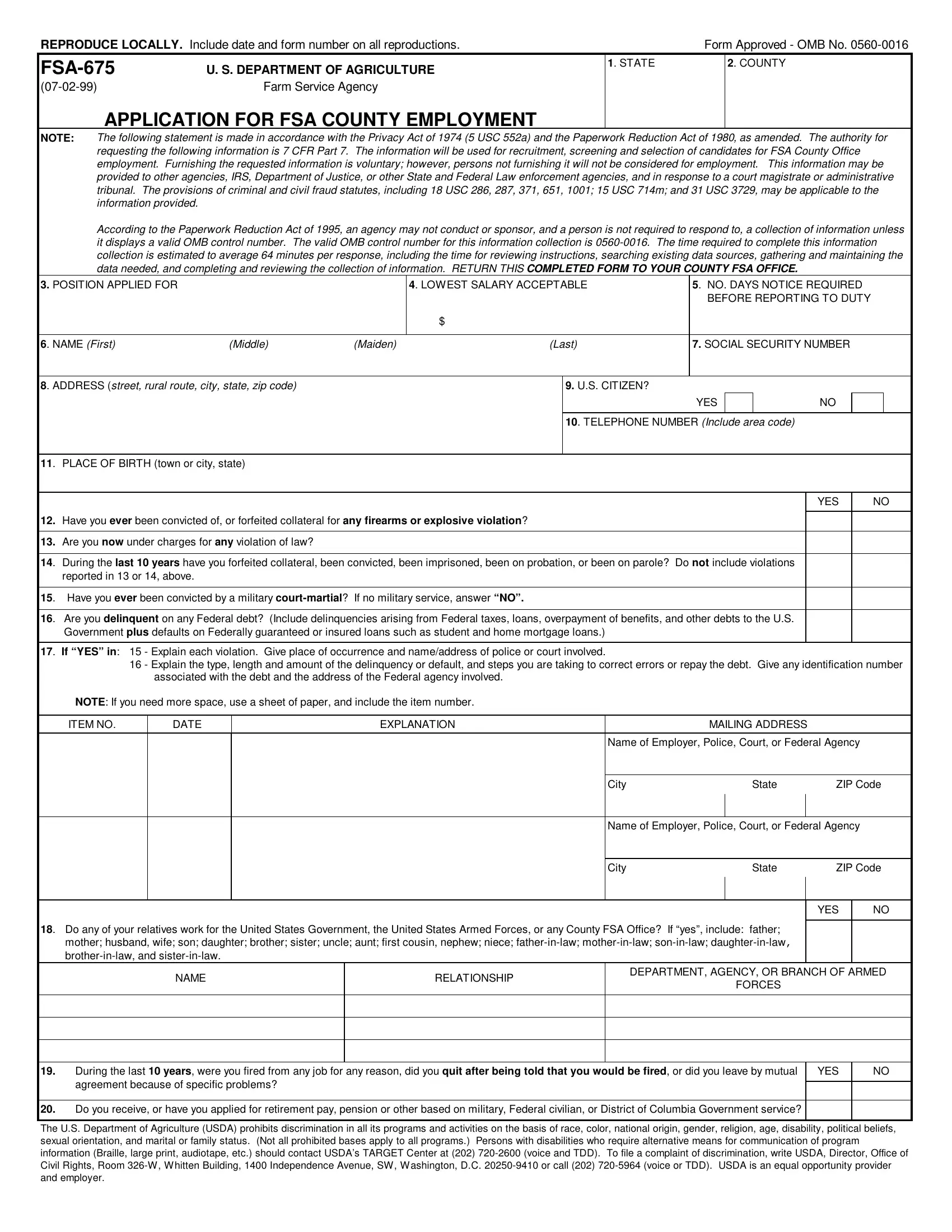
1. Start completing the 675 approved omb with a selection of necessary blanks. Note all the information you need and make sure nothing is overlooked!
2. Immediately after this section is completed, proceed to type in the relevant information in all these: Are you now under charges for any, During the last years have you, reported in or above, Have you ever been convicted by a, Are you delinquent on any Federal, Government plus defaults on, If YES in Explain each, Explain the type length and, associated with the debt and the, NOTE If you need more space use a, ITEM NO, DATE, EXPLANATION, MAILING ADDRESS, and Name of Employer Police Court or.
3. Through this step, check out NAME, RELATIONSHIP, DEPARTMENT AGENCY OR BRANCH OF, FORCES, During the last years were you, YES, Do you receive or have you applied, and The US Department of Agriculture. All of these should be filled out with utmost precision.
Those who use this document frequently make mistakes while filling out YES in this section. Be sure you review what you type in right here.
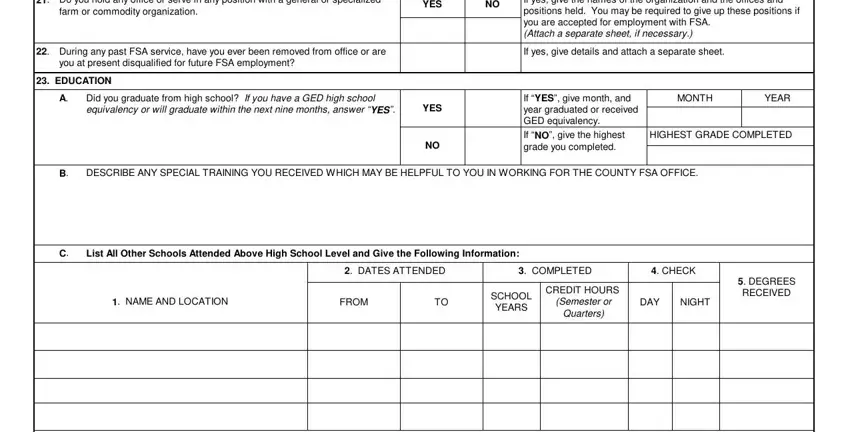
4. The subsequent part needs your attention in the subsequent areas: Do you hold any office or serve, farm or commodity organization, YES, If yes give the names of the, During any past FSA service have, If yes give details and attach a, you at present disqualified for, EDUCATION, Did you graduate from high school, YES, If YES give month and year, MONTH, YEAR, HIGHEST GRADE COMPLETED, and DESCRIBE ANY SPECIAL TRAINING YOU. Ensure you give all of the required information to move onward.
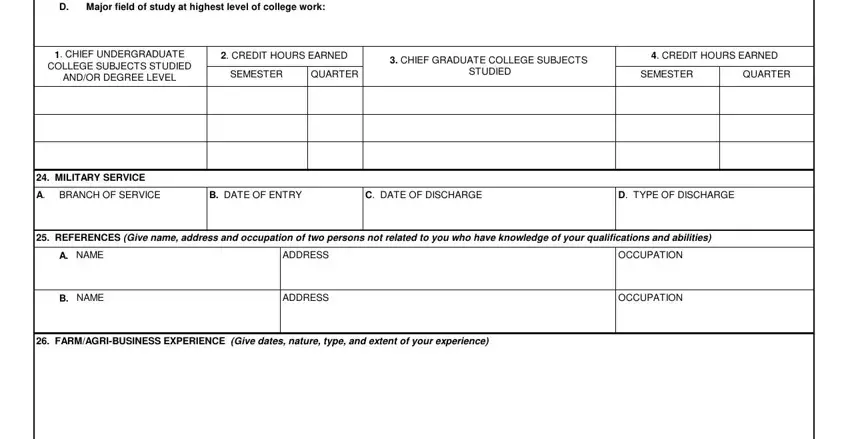
5. Now, this final segment is what you will have to finish prior to using the form. The blank fields you're looking at are the following: Major field of study at highest, CHIEF UNDERGRADUATE, COLLEGE SUBJECTS STUDIED, ANDOR DEGREE LEVEL, CREDIT HOURS EARNED, SEMESTER, QUARTER, CHIEF GRADUATE COLLEGE SUBJECTS, STUDIED, CREDIT HOURS EARNED, SEMESTER, QUARTER, MILITARY SERVICE, BRANCH OF SERVICE, and B DATE OF ENTRY.
Step 3: Confirm that the information is right and then click "Done" to conclude the process. Go for a free trial account with us and acquire direct access to 675 approved omb - downloadable, emailable, and editable in your personal account. FormsPal is committed to the privacy of our users; we make sure all information coming through our tool is secure.