Form Hcp 65 is a tax form used to calculate the amount of taxes that a company owes on its income. The form is filed annually, and must be completed by all businesses operating in the United States. The form is used to determine the company's taxable income, as well as any applicable deductions or credits. Completing Form Hcp 65 can be complex, so it is important to consult with an accountant or tax specialist before filing. Failure to submit this form can result in significant penalties and fines.
| Question | Answer |
|---|---|
| Form Name | Form Hcp 65 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | HCP 65 form hcp 65 ri |
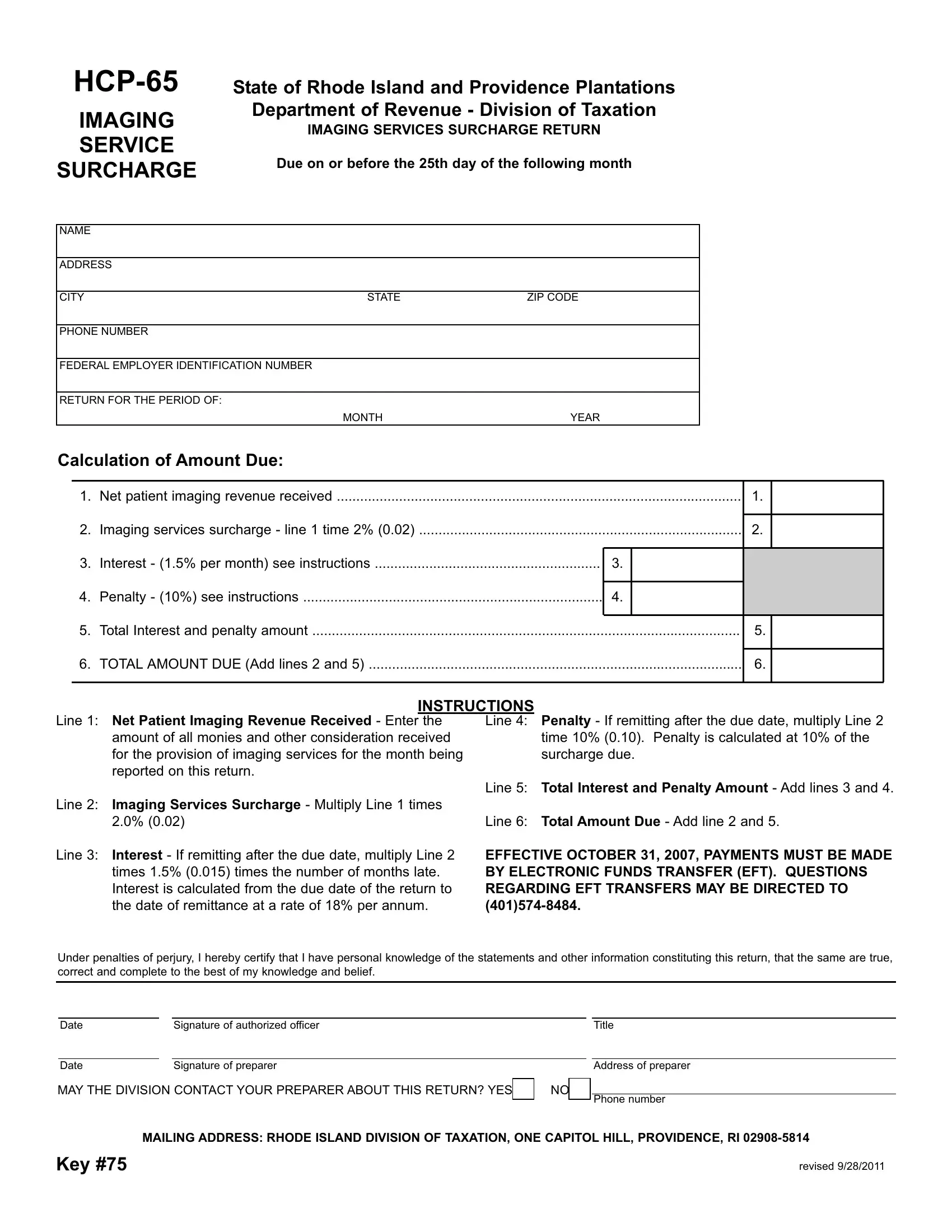
IMAGING
SERVICE
SURCHARGE
State of Rhode Island and Providence Plantations Department of Revenue - Division of Taxation
IMAGING SERVICES SURCHARGE RETURN
Due on or before the 25th day of the following month
NAME
ADDRESS
CITY |
STATE |
ZIP CODE |
PHONENUMBER
FEDERALEMPLOYERIDENTIFICATION NUMBER
RETURNFORTHEPERIOD OF:
MONTHYEAR
Calculation of Amount Due:
1. |
Net patient imaging revenuereceived |
|
1. |
|
|
|
|
|
|
|
|
2. |
Imaging services surcharge - line 1 time 2% (0.02) |
|
2. |
|
|
|
|
|
|
|
|
3. |
Interest - (1.5% per month) see instructions |
3. |
|
|
|
|
|
|
|
|
|
4. |
Penalty - (10%) see instructions |
4. |
|
|
|
|
|
|
|
|
|
5. |
Total Interest and penalty amount |
|
5. |
|
|
|
|
|
|
|
|
6. |
TOTALAMOUNTDUE(Add lines 2 and 5) |
|
6. |
|
|
|
|
|
|
|
|
INSTRUCTIONS
Line 1: Net Patient Imaging Revenue Received - Enter the amount of all monies and other consideration received for the provision of imaging services for the month being reported on this return.
Line 4: Penalty - If remitting after the due date, multiply Line 2 time 10% (0.10). Penalty is calculated at 10% of the surcharge due.
Line 2: Imaging Services Surcharge - Multiply Line 1 times 2.0% (0.02)
Line 3: Interest - If remitting after the due date, multiply Line 2 times 1.5% (0.015) times the number of months late. Interest is calculated from the due date of the return to the date of remittance at a rate of 18% per annum.
Line 5: Total Interest and Penalty Amount
Line 6: Total Amount Due
EFFECTIVE OCTOBER 31, 2007, PAYMENTS MUST BE MADE BYELECTRONIC FUNDS TRANSFER (EFT). QUESTIONS REGARDING EFT TRANSFERS MAYBE DIRECTED TO
Under penalties of perjury, I hereby certify that Ihave personal knowledge of the statements and other information constituting this return, that the same are true, correct and complete to the best of my knowledge and belief.
Date |
|
Signature of authorized officer |
|
|
|
|
|
Date |
|
Signature of preparer |
|
MAYTHE DIVISION CONTACTYOUR PREPARERABOUTTHIS RETURN? YES |
NO |
||
Title
Address of preparer
Phone number
MAILING ADDRESS:RHODE ISLAND DIVISION OF TAXATION, ONE CAPITOLHILL, PROVIDENCE,
Key #75
revised 9/28/2011