
Handling PDF documents online is actually a piece of cake with our PDF editor. You can fill out CPSP here effortlessly. FormsPal team is focused on making sure you have the absolute best experience with our tool by constantly releasing new capabilities and enhancements. Our editor has become a lot more helpful as the result of the latest updates! Currently, working with PDF documents is a lot easier and faster than ever. With a few easy steps, you are able to begin your PDF editing:
Step 1: Press the "Get Form" button in the top part of this webpage to open our PDF tool.
Step 2: With our handy PDF editing tool, you're able to do more than just fill in blanks. Express yourself and make your forms look perfect with custom textual content incorporated, or adjust the file's original content to excellence - all that supported by the capability to add any pictures and sign it off.
Concentrate while filling out this form. Make certain each blank field is filled in correctly.
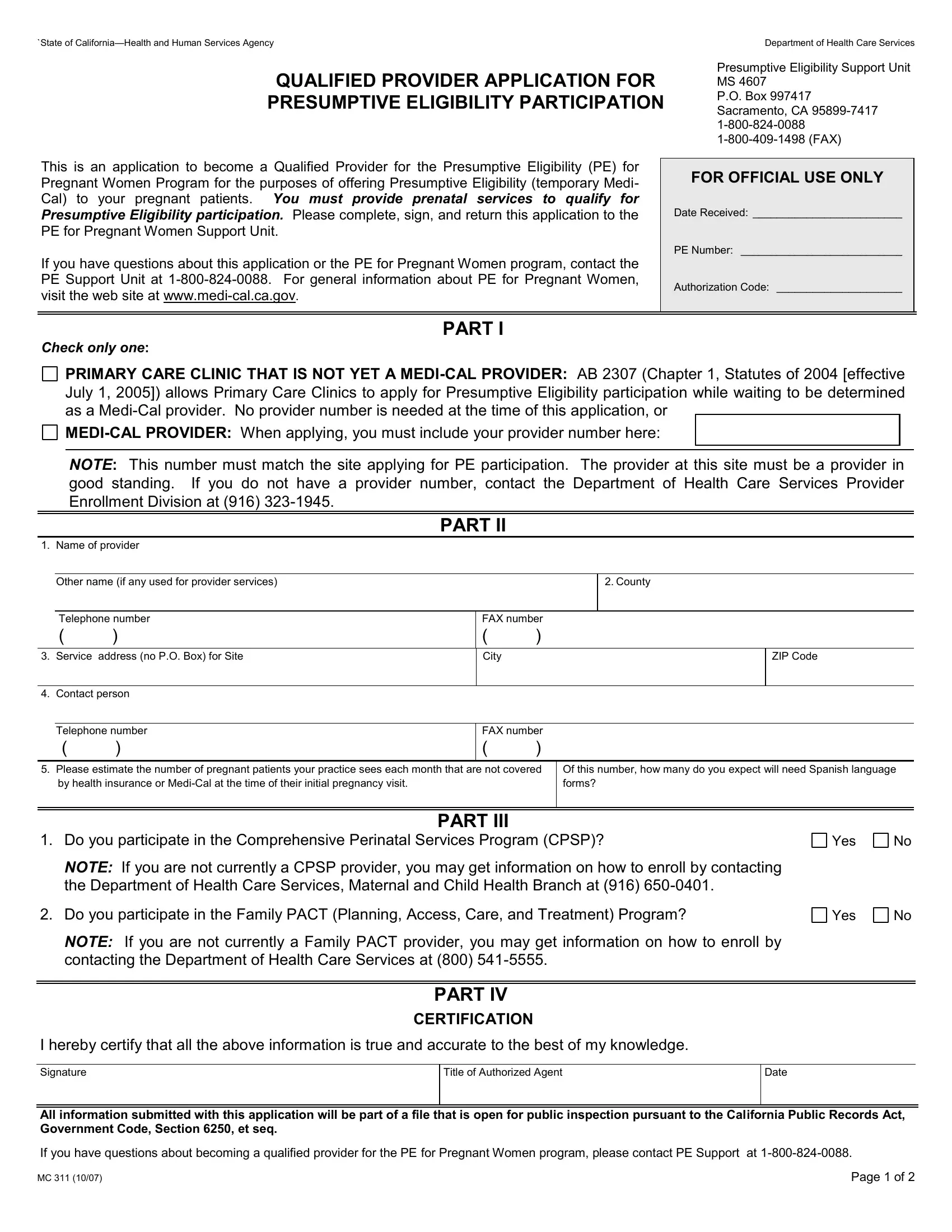
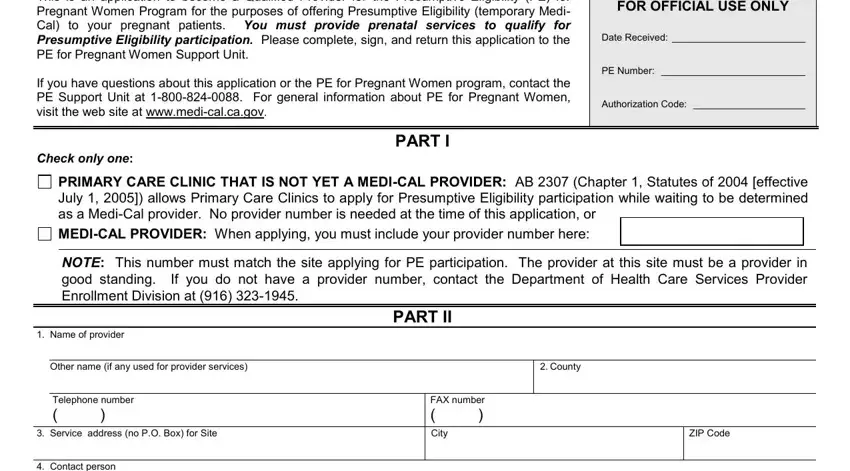
1. Start filling out your CPSP with a group of essential fields. Gather all of the necessary information and make certain not a single thing omitted!
2. Once your current task is complete, take the next step – fill out all of these fields - Contact person, Telephone number, FAX number, Please estimate the number of, by health insurance or MediCal at, Of this number how many do you, PART III, Do you participate in the, Yes, NOTE If you are not currently a, the Department of Health Care, Do you participate in the Family, Yes, NOTE If you are not currently a, and contacting the Department of with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
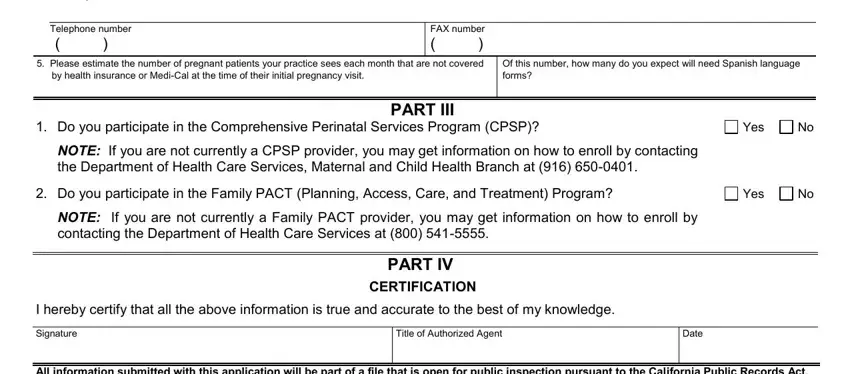
When it comes to by health insurance or MediCal at and NOTE If you are not currently a, be certain you get them right in this section. These are definitely the most significant ones in this document.
3. The following segment will be focused on notices andor further training, I print name agree to cooperate, Signature, Title of Authorized Agent, Date, and Page of - fill in each of these blanks.
Step 3: Immediately after proofreading your entries, hit "Done" and you are good to go! Join FormsPal now and immediately obtain CPSP, prepared for downloading. Every modification you make is conveniently preserved , which enables you to modify the document at a later point when required. At FormsPal.com, we aim to make sure your information is maintained protected.