

Any time you need to fill out false, there's no need to install any programs - simply make use of our online PDF editor. To keep our editor on the cutting edge of efficiency, we strive to integrate user-oriented features and improvements regularly. We are routinely glad to get feedback - play a vital part in reshaping the way you work with PDF forms. Here is what you'll need to do to get going:
Step 1: Click the "Get Form" button at the top of this page to open our editor.
Step 2: With this online PDF tool, it is easy to do more than simply fill out blank fields. Edit away and make your forms look professional with custom text incorporated, or optimize the original input to excellence - all accompanied by the capability to insert almost any images and sign it off.
It's easy to complete the pdf using this detailed guide! Here is what you need to do:
1. Fill out the false with a selection of necessary blank fields. Get all the important information and ensure there's nothing forgotten!
2. Your next step is to complete the following blank fields: Contact Person for questions, Email Address, Phone Number, Complaint Address if different, PO Box, City, State, Zip, Complaint Contact Person if, Email Address, Fax Number, Phone Number, and OCI R.
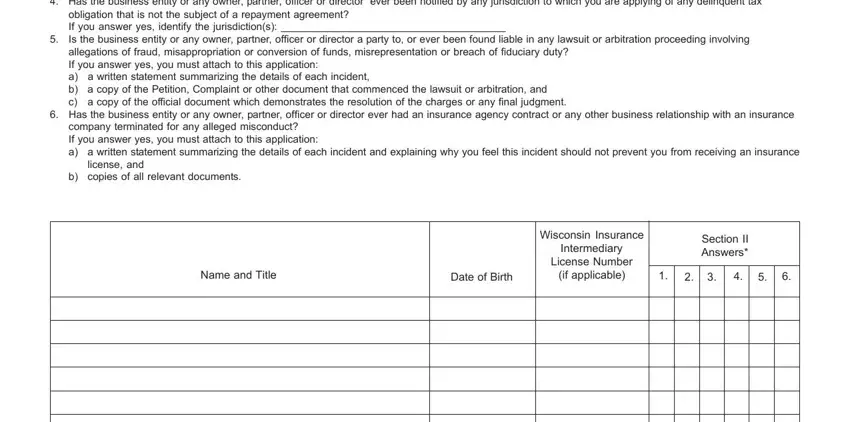
3. This next segment is considered quite simple, Has the business entity or any, obligation that is not the subject, Has the business entity or any, company terminated for any alleged, license and, b copies of all relevant documents, Name and Title, Date of Birth, Wisconsin Insurance, Intermediary, License Number, if applicable, and Section II Answers - every one of these empty fields will need to be filled in here.
4. The following paragraph needs your input in the subsequent places: OCI R. Ensure you type in all of the requested info to move further.
5. As you draw near to the finalization of this form, you'll find several more requirements that must be met. Particularly, cid Check the box and complete A, client funds or if the, A The amount of business, B The amount of business projected, C Amount of Bond required of B, bond of, cid Check the box and complete A, bank accounts, A The amount of business, B The amount of business projected, C Amount of Bond required of B, bond of, SECTION IV, FINANCIAL STATEMENT, and INSTRUCTIONS must all be done.
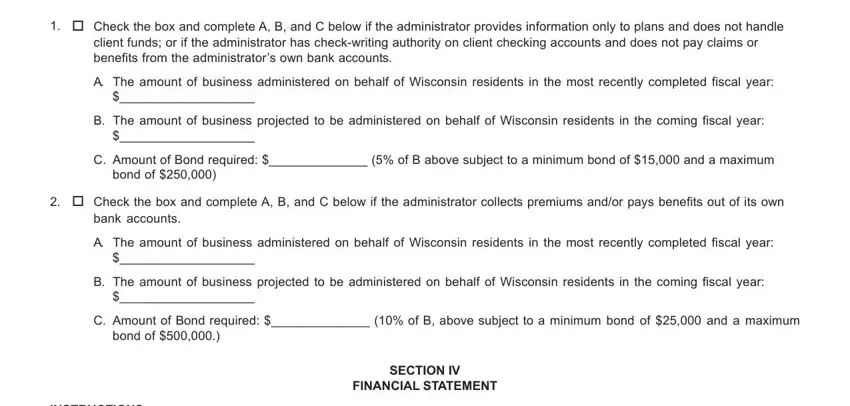
As to C Amount of Bond required of B and cid Check the box and complete A, make certain you take a second look in this section. These are certainly the key ones in this form.
Step 3: Make sure that your information is correct and then click "Done" to conclude the project. Get your false the instant you register at FormsPal for a free trial. Immediately access the form in your personal cabinet, together with any edits and changes being conveniently saved! At FormsPal, we aim to be certain that all your information is maintained protected.