CGD Form Op 336, also known as the Foreign Assistance Certification, is a United States Department of State form that must be completed by all organizations receiving foreign assistance. The form requires certifying that all funds will be used for authorized purposes and that no funds will be provided to terrorist organizations or individuals on the terrorism watch list. Completion of this form is critical for ensuring compliance with United States law and regulations governing foreign assistance. If your organization receives foreign assistance in any form - whether it's from the United States government or another source - you'll need to complete CGD Form Op 336. This form certifies that all funds received will be used for authorized purposes only, and that no funds will be provided to terrorist organizations or individuals on the terrorism watch list. Failing to complete this form could result in penalties and/or loss of funding. So make sure you're aware of all requirements an
| Question | Answer |
|---|---|
| Form Name | Form Op 336 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | SSN, DRS, overstates, Connecticut |
Department of Revenue Services |
For calendar quarter ending |
||
State of Connecticut |
|
||
PO Box 5031 |
Nursing Home User Fee |
|
|
Connecticut Tax Registration Number |
|||
Hartford CT |
Amended Return |
||
Rev.12/08 |
|
||
|
|
||
|
|
Federal Employer Identifi cation Number (FEIN) |
Complete the return in blue or black ink only.
Provider Nursing home name |
|
DRS use only |
||
|
|
|
|
|
Please |
Number and street |
PO Box |
|
|
|
|
|
||
type |
|
|
|
|
City or town |
State |
ZIP code |
||
|
||||
or print.
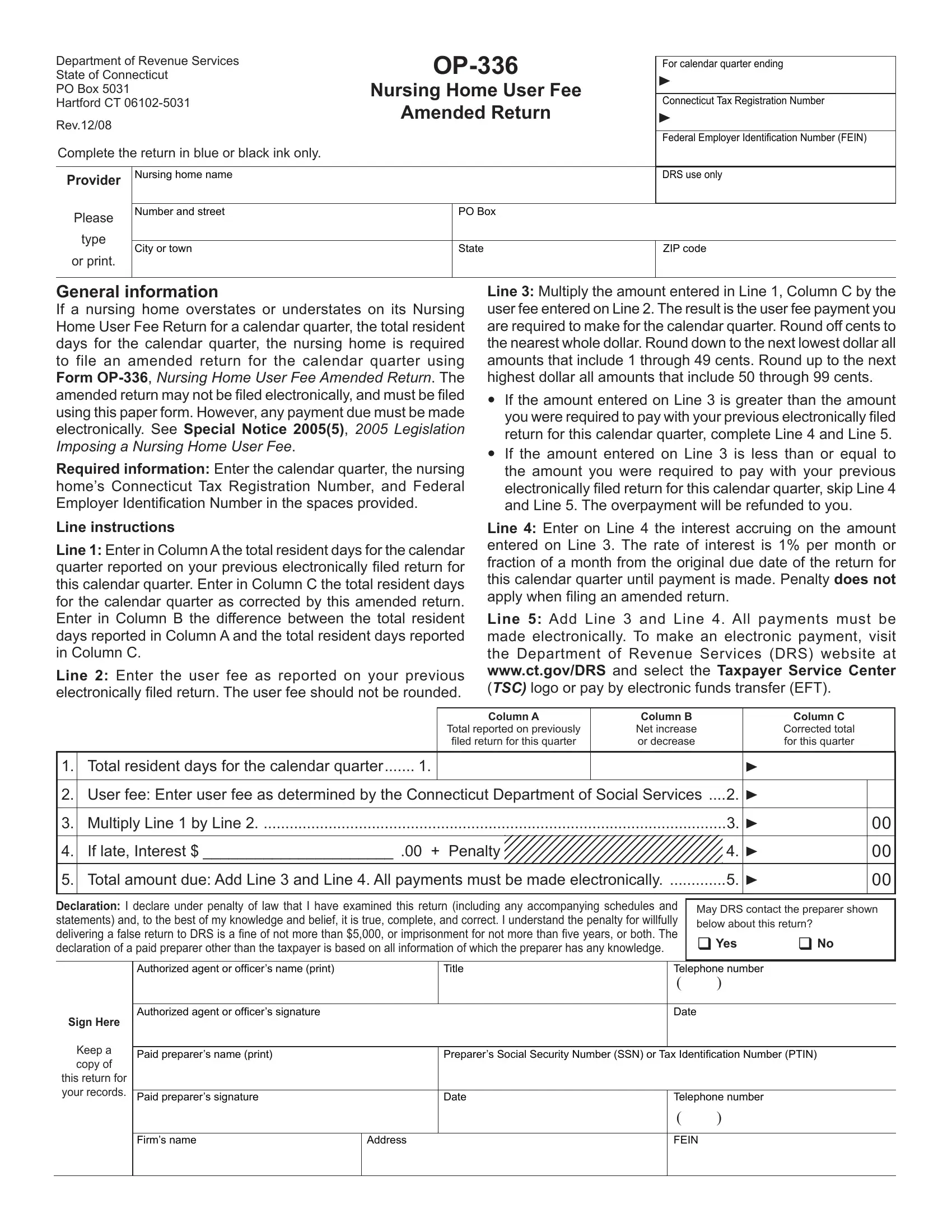
General information
If a nursing home overstates or understates on its Nursing Home User Fee Return for a calendar quarter, the total resident days for the calendar quarter, the nursing home is required to file an amended return for the calendar quarter using Form
Required information: Enter the calendar quarter, the nursing home’s Connecticut Tax Registration Number, and Federal Employer Identifi cation Number in the spaces provided.
Line instructions
Line 1: Enter in Column A the total resident days for the calendar quarter reported on your previous electronically filed return for this calendar quarter. Enter in Column C the total resident days for the calendar quarter as corrected by this amended return. Enter in Column B the difference between the total resident days reported in Column A and the total resident days reported in Column C.
Line 2: Enter the user fee as reported on your previous electronically fi led return. The user fee should not be rounded.
Line 3: Multiply the amount entered in Line 1, Column C by the user fee entered on Line 2. The result is the user fee payment you are required to make for the calendar quarter. Round off cents to the nearest whole dollar. Round down to the next lowest dollar all amounts that include 1 through 49 cents. Round up to the next highest dollar all amounts that include 50 through 99 cents.
If the amount entered on Line 3 is greater than the amount you were required to pay with your previous electronically filed return for this calendar quarter, complete Line 4 and Line 5.
If the amount entered on Line 3 is less than or equal to the amount you were required to pay with your previous electronically filed return for this calendar quarter, skip Line 4 and Line 5. The overpayment will be refunded to you.
Line 4: Enter on Line 4 the interest accruing on the amount entered on Line 3. The rate of interest is 1% per month or fraction of a month from the original due date of the return for this calendar quarter until payment is made. Penalty does not apply when fi ling an amended return.
Line 5: Add Line 3 and Line 4. All payments must be made electronically. To make an electronic payment, visit the Department of Revenue Services (DRS) website at www.ct.gov/DRS and select the Taxpayer Service Center (TSC) logo or pay by electronic funds transfer (EFT).
|
|
|
Column A |
Column B |
|
Column C |
|
|
|
|
Total reported on previously |
Net increase |
|
Corrected total |
|
|
|
|
fi led return for this quarter |
or decrease |
|
for this quarter |
|
|
|
|
|
|
|
|
|
1. |
Total resident days for the calendar quarter |
1. |
|
|
|
|
|
|
|
|
|
|
|
|
|
2. |
User fee: Enter user fee as determined by the Connecticut Department of Social Services .... |
2. |
|
|
|||
|
|
|
|
|
|
|
|
3. |
Multiply Line 1 by Line 2 |
|
|
3. |
|
00 |
|
|
|
|
|
|
|
||
4. |
If late, Interest $ ______________________ .00 + Penalty |
|
4. |
|
00 |
||
|
|
|
|
|
|||
5. |
Total amount due: Add Line 3 and Line 4. All payments must be made electronically |
5. |
|
00 |
|||
|
|
|
|
|
|
|
|
Declaration: I declare under penalty of law that I have examined this return (including any accompanying schedules and statements) and, to the best of my knowledge and belief, it is true, complete, and correct. I understand the penalty for willfully delivering a false return to DRS is a fine of not more than $5,000, or imprisonment for not more than five years, or both. The declaration of a paid preparer other than the taxpayer is based on all information of which the preparer has any knowledge.
May DRS contact the preparer shown below about this return?
Yes No
Sign Here
Keep a copy of this return for your records.
Authorized agent or officer’s name (print) |
|
Title |
Telephone number |
|
|
|
|
( |
) |
|
|
|
|
|
Authorized agent or officer’s signature |
|
|
Date |
|
|
|
|
|
|
Paid preparer’s name (print) |
|
Preparer’s Social Security Number (SSN) or Tax Identifi cation Number (PTIN) |
||
|
|
|
|
|
Paid preparer’s signature |
|
Date |
Telephone number |
|
|
|
|
( |
) |
|
|
|
|
|
Firm’s name |
Address |
|
FEIN |
|
|
|
|
|
|