
By using the online tool for PDF editing by FormsPal, it is possible to complete or alter Form Sglv 8285A right here. To maintain our editor on the forefront of convenience, we aim to put into action user-oriented capabilities and improvements regularly. We are routinely looking for feedback - help us with revampimg PDF editing. This is what you will have to do to begin:
Step 1: Click the "Get Form" button at the top of this page to open our tool.
Step 2: This editor offers you the ability to customize most PDF forms in a variety of ways. Change it by writing personalized text, adjust what's already in the PDF, and put in a signature - all within the reach of several mouse clicks!
Completing this document usually requires attention to detail. Make certain all mandatory blanks are filled in accurately.
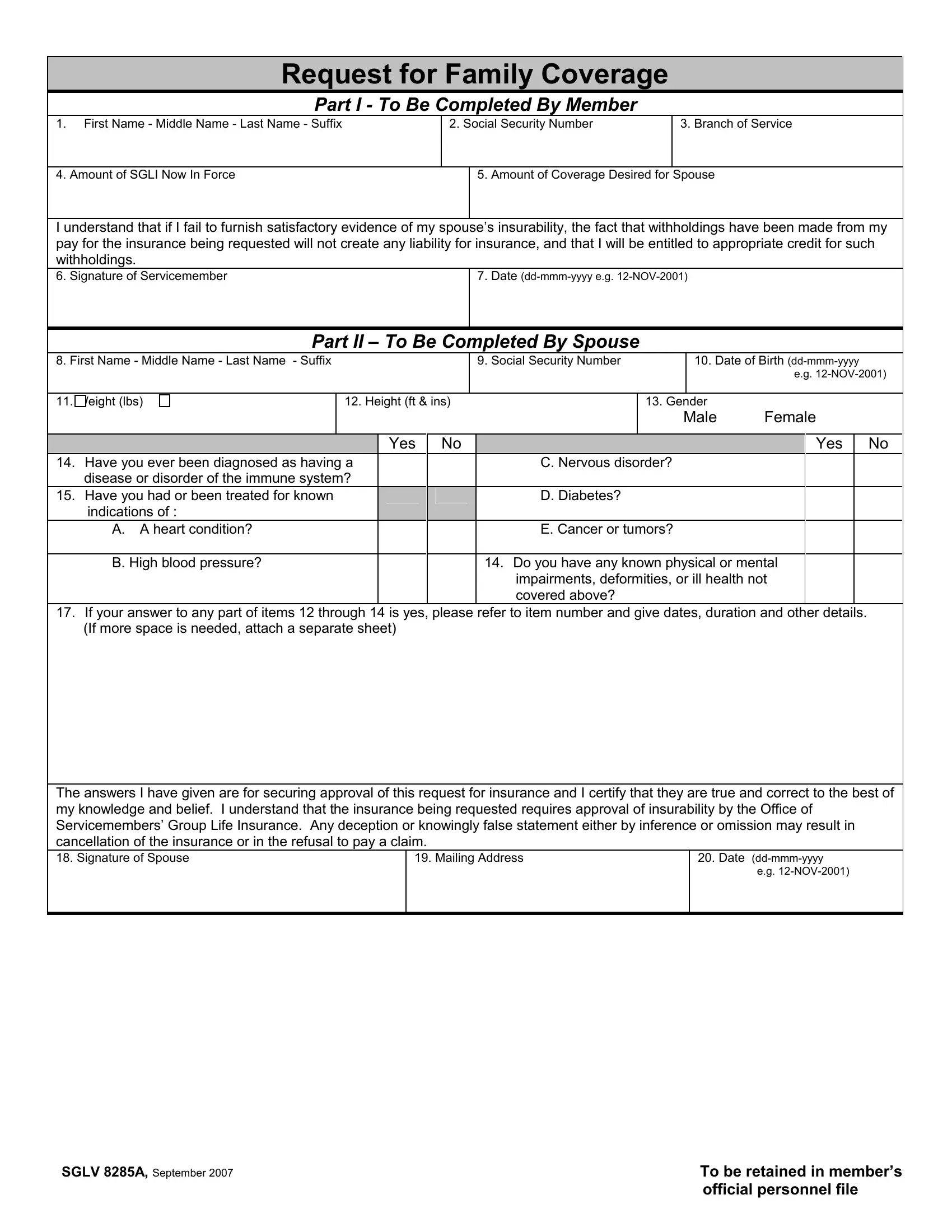
1. It is critical to complete the Form Sglv 8285A properly, thus pay close attention while filling in the parts comprising all of these fields:
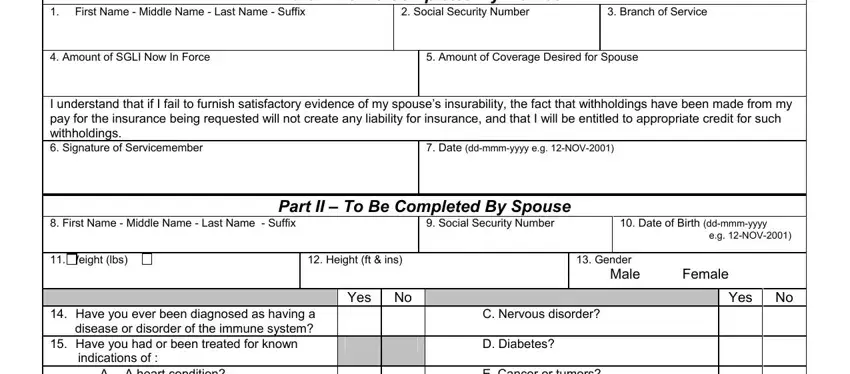
2. Just after performing this part, go to the next step and fill in the necessary particulars in all these blanks - A A heart condition B High blood, Do you have any known physical or, If your answer to any part of, Date ddmmmyyyy, Mailing Address, and eg NOV.
Regarding A A heart condition B High blood and Do you have any known physical or, be certain that you do everything right in this section. Both these are the most significant fields in this file.
3. This third part is quite easy, I certify that the signature in, Date ddmmmyyyy eg NOV, Organization and Mailing Address, Rank Title or Grade, Approve Disapprove, For OSGLI Use Only, Signature of OSGLI Representative, Date ddmmmyyyy eg NOV, INSTRUCTIONS PLEASE READ, Use this form to apply for, Family Coverage for your spouse, and TO MEMBER Complete Part I by - every one of these empty fields must be filled in here.
Step 3: Always make sure that the information is accurate and then simply click "Done" to continue further. Join FormsPal today and instantly use Form Sglv 8285A, available for download. All changes made by you are kept , letting you customize the document further if needed. FormsPal provides secure form editing without personal data record-keeping or distributing. Be assured that your data is in good hands with us!