Small Claims Court is a division of the state court system in the United States that handles civil disputes up to a specified dollar limit. The limit varies from state to state, but is typically between $2,500 and $25,000. Cases filed in Small Claims Court are usually heard by a judge without a jury. If you're considering filing a small claim, it's important to understand how Small Claims Court works and what you can expect during the process. This article will provide an overview of Small Claims Court procedure and offer some tips for preparing your case.
| Question | Answer |
|---|---|
| Form Name | Form Smcc |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | med_cert scc serious medical condition certification form |
|
|
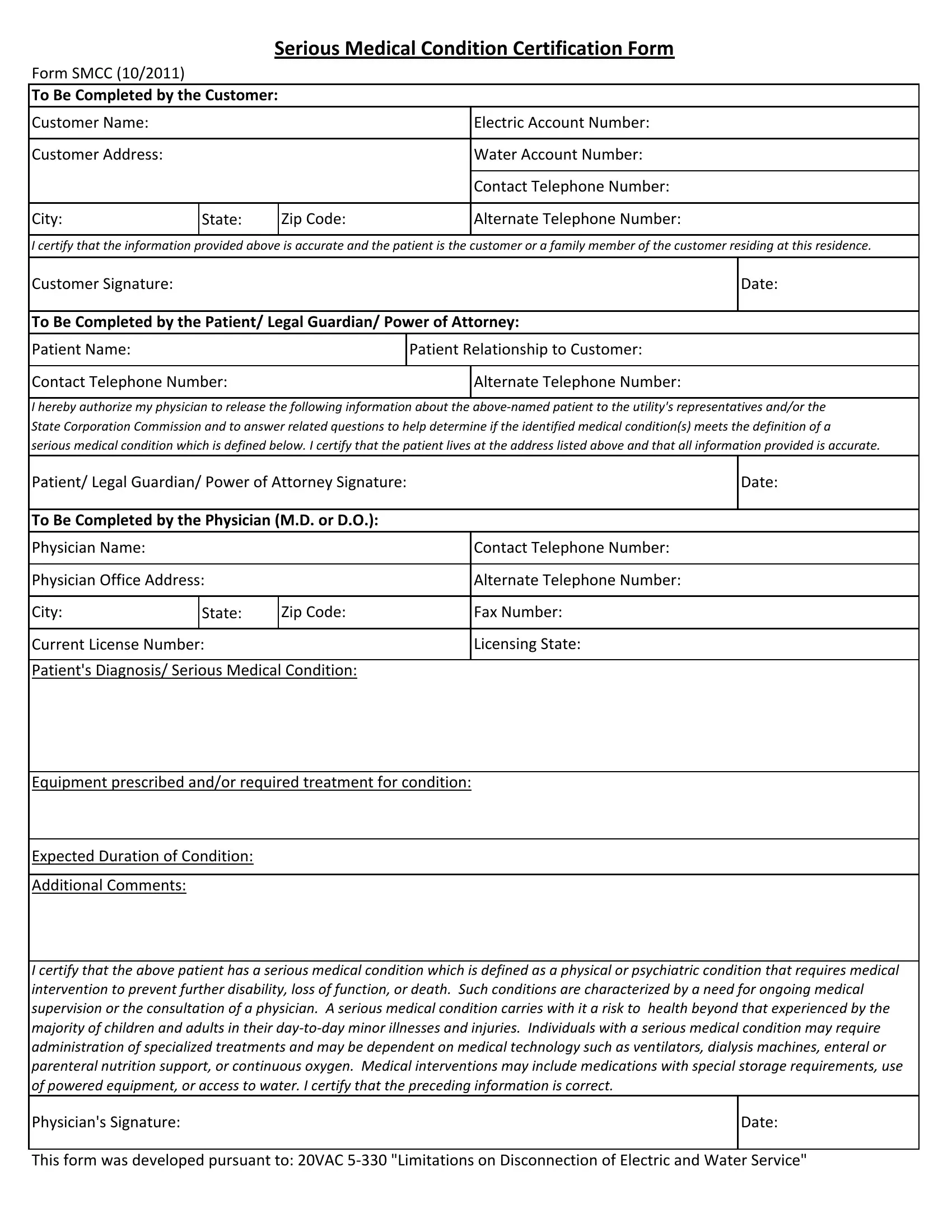
Serious Medical Condition Certification Form |
||
Form SMCC (10/2011) |
|
|
|
|
|
|
|||
To Be Completed by the Customer: |
|
|||
|
|
|
|
|
Customer Name: |
|
|
|
Electric Account Number: |
|
|
|
|
|
Customer Address: |
|
|
|
Water Account Number: |
|
|
|
|
|
|
|
|
|
Contact Telephone Number: |
|
|
|
|
|
City: |
State: |
|
Zip Code: |
Alternate Telephone Number: |
|
|
|
|
|
I certify that the information provided above is accurate and the patient is the customer or a family member of the customer residing at this residence.
Customer Signature: |
|
|
Date: |
|
|
|
|
To Be Completed by the Patient/ Legal Guardian/ Power of Attorney: |
|||
|
|
||
Patient Name: |
Patient Relationship to Customer: |
||
|
|
|
|
Contact Telephone Number: |
|
Alternate Telephone Number: |
|
|
|
|
|
I hereby authorize my physician to release the following information about the
Patient/ Legal Guardian/ Power of Attorney Signature: |
|
Date: |
||
|
|
|
|
|
To Be Completed by the Physician (M.D. or D.O.): |
|
|
||
|
|
|
|
|
Physician Name: |
|
|
Contact Telephone Number: |
|
|
|
|
||
Physician Office Address: |
|
Alternate Telephone Number: |
||
|
|
|
|
|
City: |
State: |
Zip Code: |
Fax Number: |
|
|
|
|
|
|
Current License Number: |
|
Licensing State: |
||
|
|
|
|
|
Patient's Diagnosis/ Serious Medical Condition: |
|
|
||
Equipment prescribed and/or required treatment for condition:
Expected Duration of Condition:
Additional Comments:
I certify that the above patient has a serious medical condition which is defined as a physical or psychiatric condition that requires medical intervention to prevent further disability, loss of function, or death. Such conditions are characterized by a need for ongoing medical supervision or the consultation of a physician. A serious medical condition carries with it a risk to health beyond that experienced by the majority of children and adults in their
Physician's Signature: |
Date: |
|
|
This form was developed pursuant to: 20VAC