
Should you desire to fill out Form Spb 810 Be, there's no need to download any programs - simply use our PDF tool. In order to make our editor better and simpler to work with, we continuously come up with new features, taking into consideration feedback coming from our users. To start your journey, go through these easy steps:
Step 1: Click the "Get Form" button in the top area of this webpage to access our tool.
Step 2: With our online PDF file editor, you can do more than simply complete forms. Edit away and make your docs look faultless with custom textual content added, or modify the original content to excellence - all accompanied by an ability to incorporate stunning photos and sign the file off.
It is actually simple to finish the pdf with this practical tutorial! This is what you want to do:
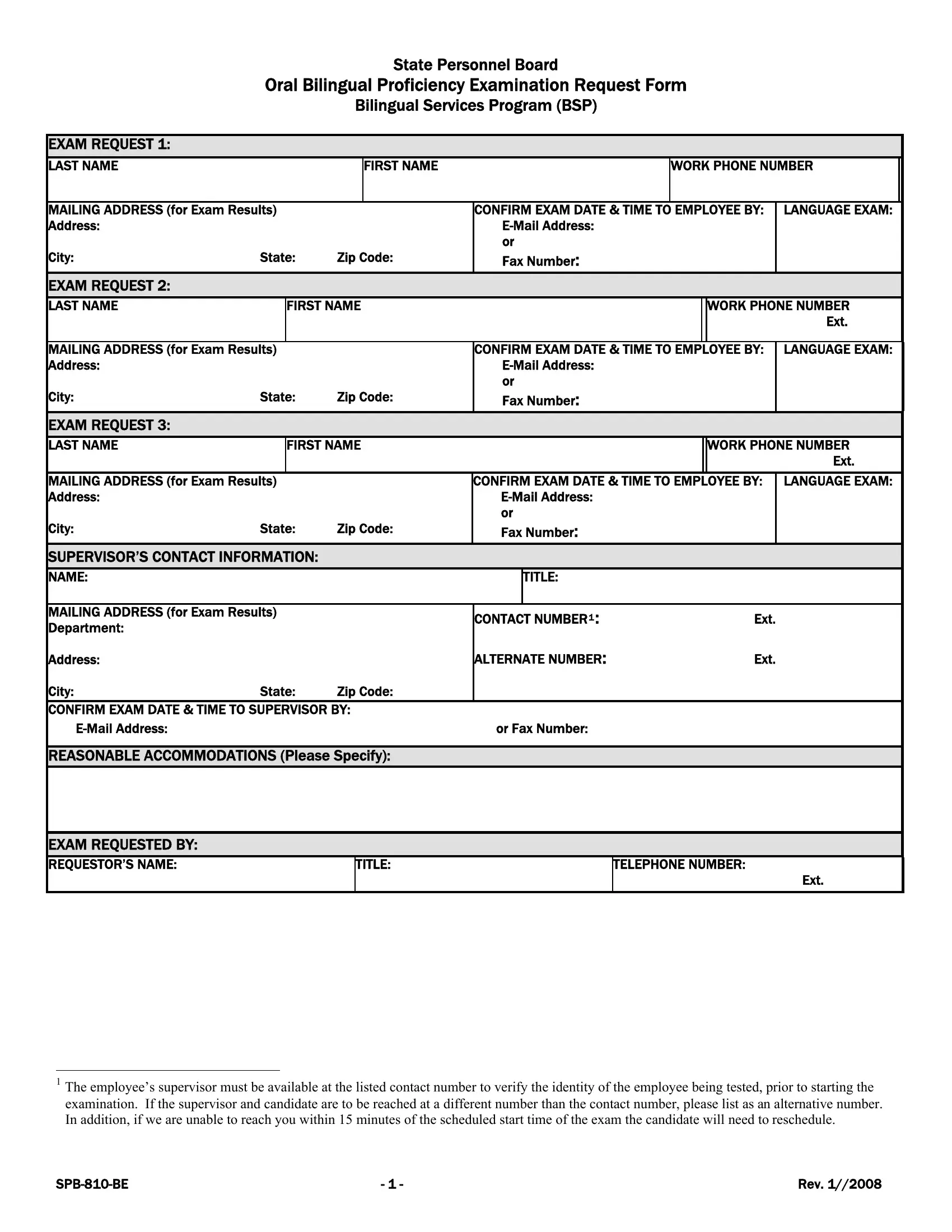
1. Complete your Form Spb 810 Be with a group of necessary blanks. Consider all of the required information and ensure nothing is neglected!
Step 3: Prior to submitting the form, you should make sure that all blanks were filled out the proper way. As soon as you’re satisfied with it, click “Done." After starting a7-day free trial account at FormsPal, you will be able to download Form Spb 810 Be or send it via email immediately. The PDF file will also be readily available in your personal account menu with your every change. FormsPal provides protected form editor without data recording or distributing. Feel safe knowing that your information is in good hands here!