Form Ui1 is a widget that can be used to gather user input. It is customizable and easy to use, making it perfect for any project. This widget is perfect for collecting feedback from your users, or for gathering any other type of user input. Thanks to its flexibility and ease of use, you'll be able to create stunning form widgets with little effort. So why not give Form Ui1 a try today? You won't be disappointed.
| Question | Answer |
|---|---|
| Form Name | Form Ui1 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | montana ui, PROPRIETORSHIP, UI, FEIN |
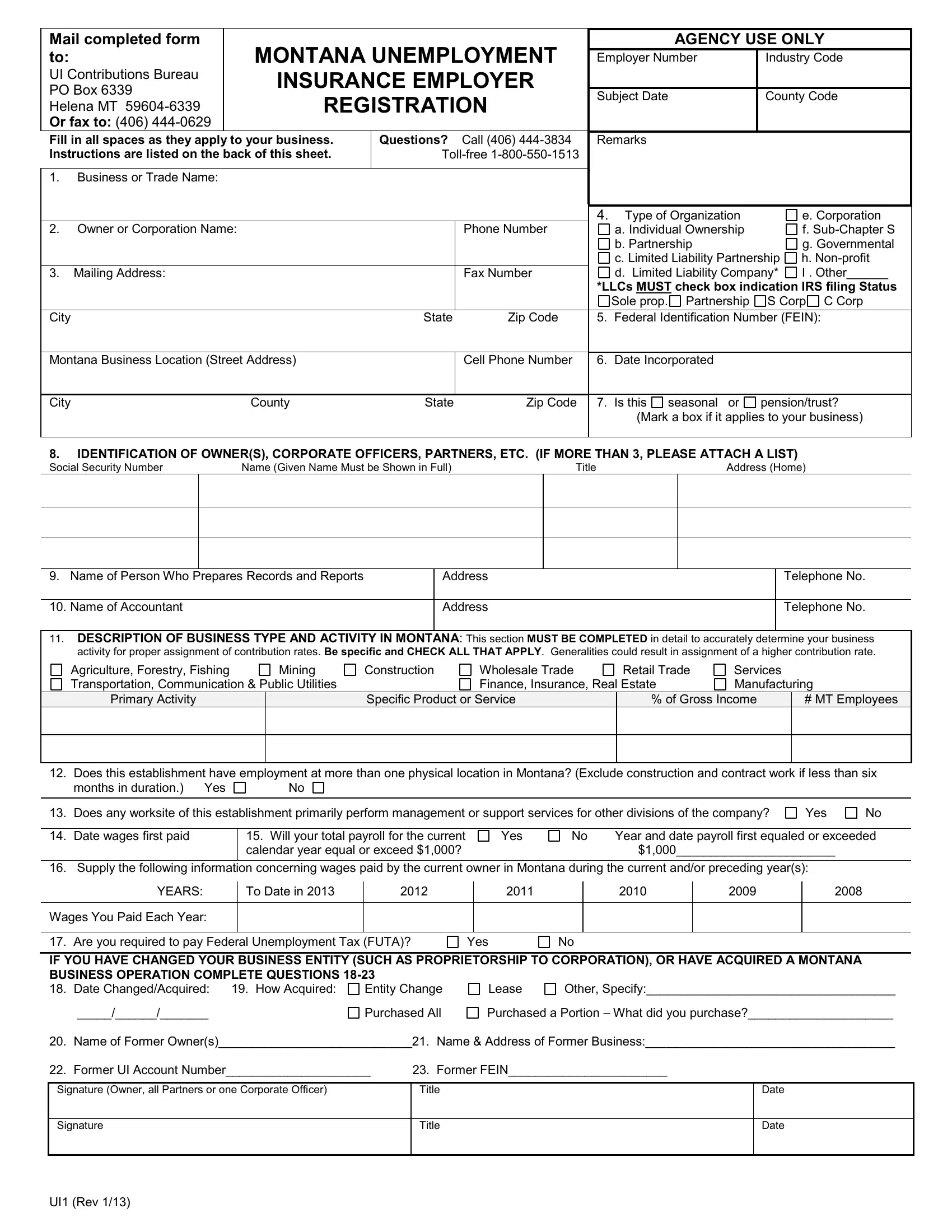
Mail completed form |
MONTANA UNEMPLOYMENT |
|
AGENCY USE ONLY |
||
to: |
|
Employer Number |
Industry Code |
||
UI Contributions Bureau |
INSURANCE EMPLOYER |
|
|
|
|
PO Box 6339 |
|
|
|
||
REGISTRATION |
|
Subject Date |
County Code |
||
Helena MT |
|
||||
|
|
|
|||
Or fax to: (406) |
|
|
|
|
|
Fill in all spaces as they apply to your business. |
Questions? Call (406) |
|
Remarks |
|
|
Instructions are listed on the back of this sheet. |
|
|
|
||
|
|
|
|
|
|
1.Business or Trade Name:
|
|
|
|
4. |
Type of Organization |
|
e. Corporation |
|
2. Owner or Corporation Name: |
|
Phone Number |
|
a. Individual Ownership |
|
f. |
||
|
|
|
|
|
b. Partnership |
|
g. Governmental |
|
|
|
|
|
|
c. Limited Liability Partnership |
h. |
||
3. |
Mailing Address: |
|
Fax Number |
|
d. Limited Liability Company* |
I . Other______ |
||
|
|
|
|
*LLCs MUST check box indication IRS filing Status |
||||
|
|
|
|
|
Sole prop. |
Partnership |
S Corp C Corp |
|
City |
|
State |
Zip Code |
5. |
Federal Identification Number (FEIN): |
|||
|
|
|
|
|
|
|
||
Montana Business Location (Street Address) |
|
Cell Phone Number |
6. |
Date Incorporated |
|
|
||
|
|
|
|
|
|
|
|
|
City |
County |
State |
Zip Code |
7. |
Is this |
seasonal or |
pension/trust? |
|
|
|
|
|
|
(Mark a box if it applies to your business) |
|||
|
|
|
|
|
|
|
|
|
8.IDENTIFICATION OF OWNER(S), CORPORATE OFFICERS, PARTNERS, ETC. (IF MORE THAN 3, PLEASE ATTACH A LIST)
Social Security Number |
Name (Given Name Must be Shown in Full) |
Title |
Address (Home) |
9. |
Name of Person Who Prepares Records and Reports |
Address |
10. |
Name of Accountant |
Address |
|
|
|
Telephone No.
Telephone No.
11.DESCRIPTION OF BUSINESS TYPE AND ACTIVITY IN MONTANA: This section MUST BE COMPLETED in detail to accurately determine your business activity for proper assignment of contribution rates. Be specific and CHECK ALL THAT APPLY. Generalities could result in assignment of a higher contribution rate.
Agriculture, Forestry, Fishing |
Mining |
Construction |
Wholesale Trade |
Retail Trade |
Services |
|
|
Transportation, Communication & Public Utilities |
|
Finance, Insurance, Real Estate |
Manufacturing |
||||
Primary Activity |
|
Specific Product or Service |
% of Gross Income |
|
# MT Employees |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
12. Does this establishment have employment at more than one physical location in Montana? (Exclude construction and contract work if less than six
months in duration.) Yes |
No |
|
|
13. Does any worksite of this establishment primarily perform management or support services for other divisions of the company?
Yes
No
14. Date wages first paid
15.Will your total payroll for the current calendar year equal or exceed $1,000?
Yes
No |
Year and date payroll first equaled or exceeded |
|
$1,000_______________________ |
16. Supply the following information concerning wages paid by the current owner in Montana during the current and/or preceding year(s):
YEARS: |
To Date in 2013 |
2012 |
2011 |
2010 |
2009 |
2008 |
Wages You Paid Each Year:
17. Are you required to pay Federal Unemployment Tax (FUTA)?
Yes
No
IF YOU HAVE CHANGED YOUR BUSINESS ENTITY (SUCH AS PROPRIETORSHIP TO CORPORATION), OR HAVE ACQUIRED A MONTANA
BUSINESS OPERATION COMPLETE QUESTIONS |
|
|
|
|
||
18. |
Date Changed/Acquired: 19. How Acquired: |
Entity Change |
Lease |
Other, Specify:____________________________________ |
||
|
_____/______/_______ |
Purchased All |
Purchased a Portion – What did you purchase?_____________________ |
|||
20. |
Name of Former Owner(s)____________________________21. |
Name & Address of Former Business:____________________________________ |
||||
22. |
Former UI Account Number_____________________ |
23. |
Former FEIN_______________________ |
|||
Signature (Owner, all Partners or one Corporate Officer)
Title
Date
Signature
Title
Date
UI1 (Rev 1/13)