
DBA can be filled in without any problem. Just try FormsPal PDF editing tool to get it done without delay. FormsPal team is focused on providing you with the perfect experience with our editor by regularly releasing new functions and improvements. With these updates, using our tool becomes easier than ever before! Getting underway is effortless! What you need to do is take the next basic steps below:
Step 1: Access the PDF in our editor by clicking on the "Get Form Button" at the top of this page.
Step 2: With this advanced PDF editing tool, you could do more than simply fill out forms. Edit away and make your documents look perfect with customized textual content added, or modify the original input to excellence - all that supported by an ability to insert your own photos and sign the file off.
This PDF will require specific information to be filled out, so you must take the time to type in precisely what is expected:
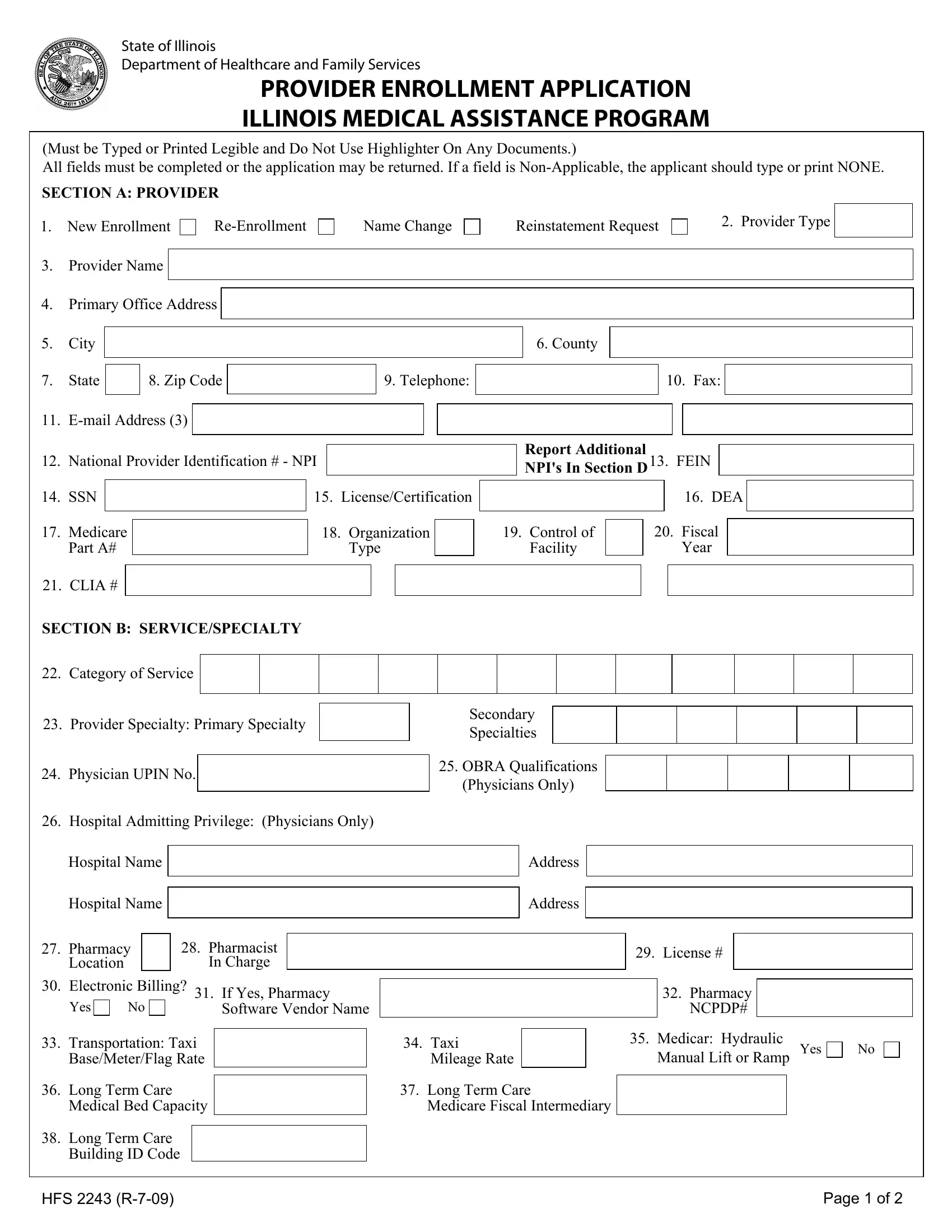
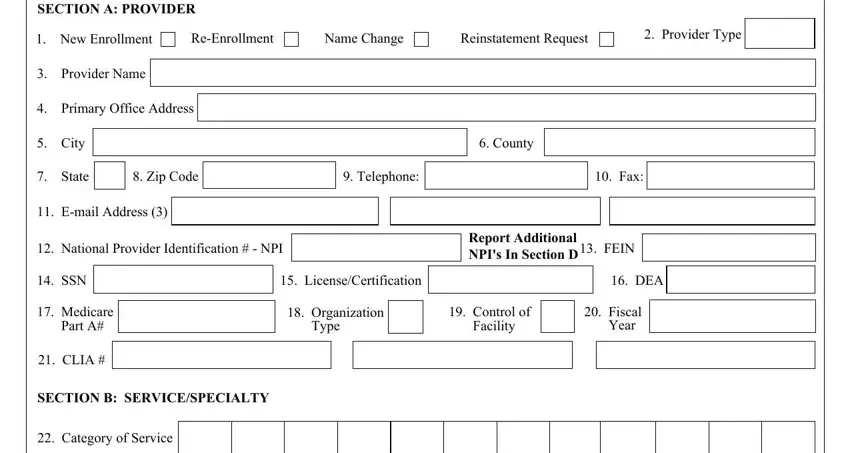
1. For starters, once filling out the DBA, beging with the page that has the next blank fields:
2. Now that the previous segment is finished, it's time to insert the required details in Provider Specialty Primary, Physician UPIN No, Hospital Admitting Privilege, Hospital Name, Hospital Name, Secondary Specialties, OBRA Qualifications Physicians, Address, Address, Pharmacy Location, Pharmacist In Charge, Electronic Billing, Yes, If Yes Pharmacy Software Vendor, and License allowing you to move on further.
3. The third step is simple - fill out all the fields in Long Term Care Building ID Code, HFS R, and Page of in order to finish this part.

4. To move forward, the following stage involves filling in a handful of empty form fields. Included in these are SECTION C FORMER PARTICIPATION, Change of Ownership, Yes, Former Provider Number, Former Provider Name, SECTION D ADDITIONAL NPI National, NPI, NPI, NPI, NPI, SECTION E PAYEE INFORMATION, Effective Date, NPI, NPI, and Telephone, which are key to carrying on with this process.
5. Since you approach the conclusion of the form, there are actually a few extra requirements that should be satisfied. Particularly, SSNFEIN, Billing ProviderPay To NPI, Medicare Part B, PIN, DMERC, Name, DBA, Street Address, City, SSNFEIN, Telephone, State, Zip Code, TIN Type Code, and Billing ProviderPay To NPI should be filled out.
People frequently make errors when completing Street Address in this area. Be sure to double-check whatever you type in here.
Step 3: Before moving forward, make sure that all blank fields were filled out as intended. The moment you confirm that it's correct, click on “Done." Get the DBA the instant you subscribe to a 7-day free trial. Easily access the pdf file within your personal account, with any edits and adjustments automatically preserved! FormsPal guarantees protected document completion devoid of personal data recording or distributing. Rest assured that your details are in good hands here!