Are you an employer who is unfamiliar with Form 28M 11? Have you been having difficulty keeping up with the mandates and deadlines established by the Canadian government? It’s essential that employers understand their obligations to keep their companies compliant — information regarding mandated filings may be difficult to navigate for those new to managerial duties. That’s why we are here to help: our blog post covers everything you need to know about Form 28M 11. In this article, we will discuss what form must be completed, when it must be filed, and how accurate reporting can prevent unnecessary delays. Read on for all of the details!
| Question | Answer |
|---|---|
| Form Name | Mandated Form 28M 11 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | MCDHH, 2009, SSN, SSDI |
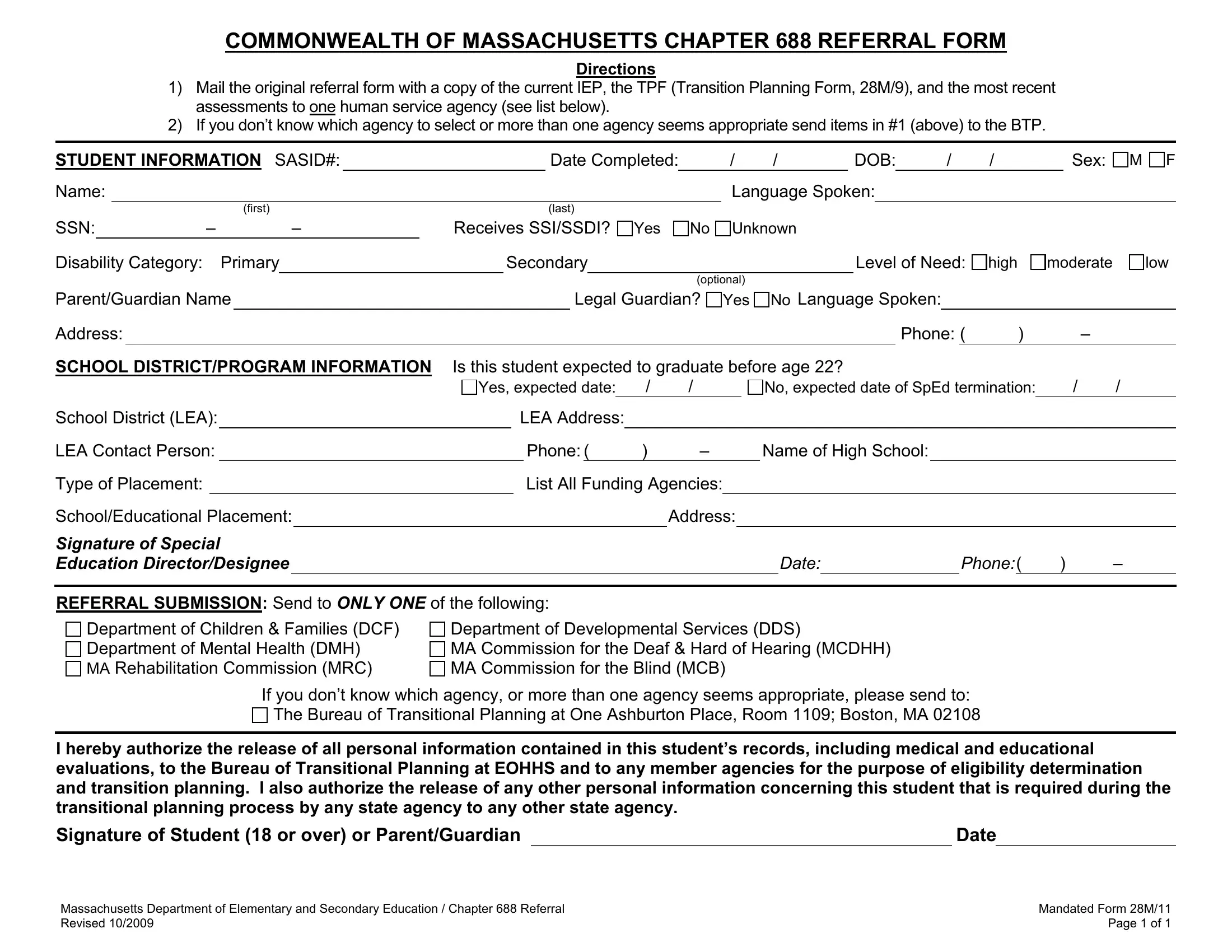
COMMONWEALTH OF MASSACHUSETTS CHAPTER 688 REFERRAL FORM
Directions
1)Mail the original referral form with a copy of the current IEP, the TPF (Transition Planning Form, 28M/9), and the most recent assessments to one human service agency (see list below).
2)If you don’t know which agency to select or more than one agency seems appropriate send items in #1 (above) to the BTP.
STUDENT INFORMATION SASID#: |
|
Date Completed: |
/ |
/ |
DOB: |
/ |
/ |
Sex: |
|||
|
|
|
|
|
|
|
|
|
|
|
|
Name: |
|
|
|
Language Spoken: |
|
|
|
||||
|
(first) |
|
(last) |
|
|
|
|
|
|
|
|
M F
SSN: |
|
– |
|
– |
Receives SSI/SSDI? Yes |
No Unknown |
|||
Disability Category: |
|
Primary |
|
Secondary |
|
Level of Need: |
|||
|
|
|
|
|
|
|
|
(optional) |
|
high
moderate
low
Parent/Guardian Name |
|
Legal Guardian? |
Address:
Yes No Language Spoken:
Phone: ( ) –
SCHOOL DISTRICT/PROGRAM INFORMATION |
Is this student expected to graduate before age 22? |
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
Yes, expected date: |
|
/ |
/ |
|
|
|
No, expected date of SpEd termination: |
/ |
/ |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
School District (LEA): |
|
|
LEA Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
LEA Contact Person: |
|
|
|
Phone:( |
|
) |
– |
|
Name of High School: |
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Type of Placement: |
|
|
|
|
List All Funding Agencies: |
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
School/Educational Placement: |
|
|
|
|
|
|
|
|
Address: |
|
|
|
|
|
|
|
|
|
|
|
||||
Signature of Special |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Education Director/Designee |
|
|
|
|
|
|
|
|
|
|
|
|
DATE: |
|
PHONE:( |
) |
– |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
REFERRAL SUBMISSION: Send to ONLY ONE of the following:
Department of Children & Families (DCF)
Department of Mental Health (DMH)
MA Rehabilitation Commission (MRC)
Department of Developmental Services (DDS)
MA Commission for the Deaf & Hard of Hearing (MCDHH) MA Commission for the Blind (MCB)
If you don’t know which agency, or more than one agency seems appropriate, please send to:
The Bureau of Transitional Planning at One Ashburton Place, Room 1109; Boston, MA 02108
I hereby authorize the release of all personal information contained in this student’s records, including medical and educational evaluations, to the Bureau of Transitional Planning at EOHHS and to any member agencies for the purpose of eligibility determination and transition planning. I also authorize the release of any other personal information concerning this student that is required during the transitional planning process by any state agency to any other state agency.
Signature of Student (18 or over) or Parent/Guardian |
|
Date |
|
|
|
|
|
Massachusetts Department of Elementary and Secondary Education / Chapter 688 Referral |
Mandated Form 28M/11 |
Revised 10/2009 |
Page 1 of 1 |