Have you recently launched a business in Marshall County that requires an Occupational License Tax Form? Are you looking to understand the ins and outs of this complex filing process? You've come to the right place! In this blog post, we'll cover all aspects of the Marshall County Occupational License Tax Form. From why it's required to how long processing can take, we'll guide you through every step so you can complete your form with ease.
| Question | Answer |
|---|---|
| Form Name | Marshall County Occupational License Tax Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | marshall county occupational tax form, marshall county occupational license tax, marshall county ky occupational tax, occupation |
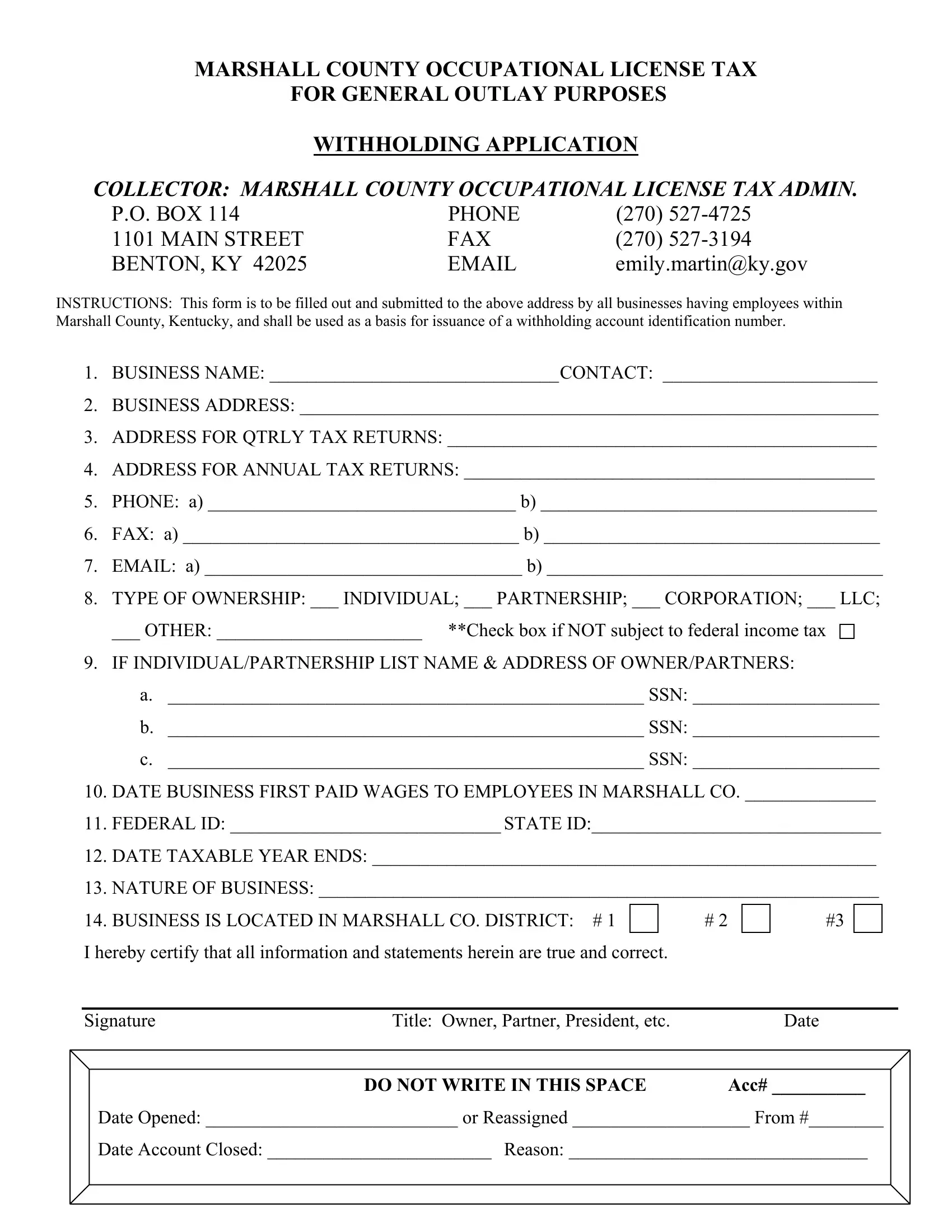
MARSHALL COUNTY OCCUPATIONAL LICENSE TAX
FOR GENERAL OUTLAY PURPOSES
WITHHOLDING APPLICATION
COLLECTOR: MARSHALL COUNTY OCCUPATIONAL LICENSE TAX ADMIN.
P.O. BOX 114 |
PHONE |
(270) |
1101 MAIN STREET |
FAX |
(270) |
BENTON, KY 42025 |
emily.martin@ky.gov |
INSTRUCTIONS: This form is to be filled out and submitted to the above address by all businesses having employees within Marshall County, Kentucky, and shall be used as a basis for issuance of a withholding account identification number.
1.BUSINESS NAME: _______________________________CONTACT: _______________________
2.BUSINESS ADDRESS: ______________________________________________________________
3.ADDRESS FOR QTRLY TAX RETURNS: ______________________________________________
4.ADDRESS FOR ANNUAL TAX RETURNS: ____________________________________________
5.PHONE: a) _________________________________ b) ____________________________________
6.FAX: a) ____________________________________ b) ____________________________________
7.EMAIL: a) __________________________________ b) ____________________________________
8.TYPE OF OWNERSHIP: ___ INDIVIDUAL; ___ PARTNERSHIP; ___ CORPORATION; ___ LLC;
___ OTHER: ______________________ **Check box if NOT subject to federal income tax
9.IF INDIVIDUAL/PARTNERSHIP LIST NAME & ADDRESS OF OWNER/PARTNERS:
a.___________________________________________________ SSN: ____________________
b.___________________________________________________ SSN: ____________________
c.___________________________________________________ SSN: ____________________
10.DATE BUSINESS FIRST PAID WAGES TO EMPLOYEES IN MARSHALL CO. ______________
11.FEDERAL ID: _____________________________ STATE ID:_______________________________
12.DATE TAXABLE YEAR ENDS: ______________________________________________________
13.NATURE OF BUSINESS: ____________________________________________________________
14. BUSINESS IS LOCATED IN MARSHALL CO. DISTRICT: # 1 |
# 2 |
#3 |
|
I hereby certify that all information and statements herein are true and correct. |
|
|
|
|
|
|
|
Signature |
Title: Owner, Partner, President, etc. |
|
Date |
|
DO NOT WRITE IN THIS SPACE |
|
ACC# __________ |
Date Opened: ___________________________ or Reassigned ___________________ From #________
Date Account Closed: ________________________ Reason: ________________________________