Are you a Maryland resident who is looking to make a state-related insurance claim? Filing the correct paperwork can be confusing and complicated. To help simplify the process for you, this blog post will provide all of the essential information that you need to understand about the official Maryland State Claim Form. From detailed filing instructions to assistance if your form gets rejected or lost in transit, this guide is designed to serve as an easy-to-follow reference for submitting insurance claims on behalf of yourself or someone else in the state of Maryland.
| Question | Answer |
|---|---|
| Form Name | Maryland State Claim Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | maryland employees claim form, maryland state of claim form, maryland health claim, md state of claim form |
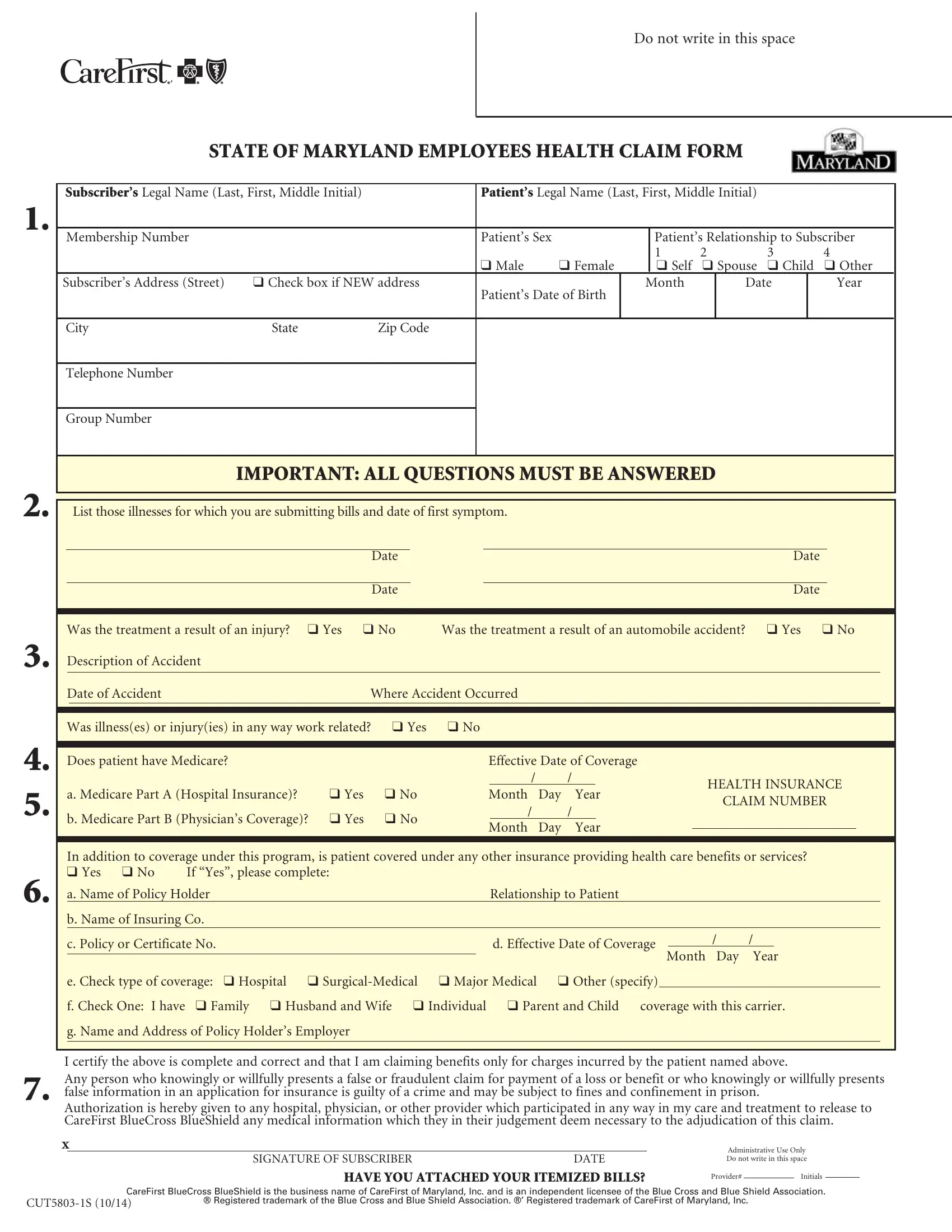
Do not write in this space
STATE OF MARYLAND EMPLOYEES HEALTH CLAIM FORM
1.
2.
3.
4.
5.
6.
7.
Subscriber’s Legal Name (Last, First, Middle Initial) |
|
Patient’s Legal Name (Last, First, Middle Initial) |
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|||
Membership Number |
|
|
Patient’s Sex |
|
|
Patient’s Relationship to Subscriber |
|
|||||
|
|
|
|
|
|
1 |
2 |
|
3 |
|
4 |
|
|
|
|
q Male |
q Female |
|
q Self |
q Spouse |
q Child |
q Other |
|
||
Subscriber’s Address (Street) |
q Check box if NEW address |
Patient’s Date of Birth |
Month |
|
Date |
|
Year |
|
||||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
State |
Zip Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Telephone Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Group Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
IMPORTANT: ALL QUESTIONS MUST BE ANSWERED
|
|
List those illnesses for which you are submitting bills and date of first symptom. |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date |
|
|
|
|
|
|
|
|
|
|
|
Date |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
Date |
|
|
|
|
|
|
|
|
|
|
|
Date |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Was the treatment a result of an injury? |
q Yes q No |
Was the treatment a result of an automobile accident? |
q Yes q No |
|
|||||||||||||||||
|
Description of Accident |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Date of Accident |
|
Where Accident Occurred |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Was illness(es) or injury(ies) in any way work related? |
q Yes |
q No |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Does patient have Medicare? |
|
|
|
|
|
Effective Date of Coverage |
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
/ |
|
/ |
|
|
|
HEALTH INSURANCE |
|
|||||||
|
a. Medicare Part A (Hospital Insurance)? |
q Yes |
q No |
|
|
Month |
Day |
Year |
|
|
|
|||||||||||
|
|
|
|
|
CLAIM NUMBER |
|
||||||||||||||||
|
|
|
|
|
|
|
|
/ |
|
/ |
|
|
|
|
||||||||
|
b. Medicare Part B (Physician’s Coverage)? q Yes |
q No |
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
Month |
Day |
Year |
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
In addition to coverage under this program, is patient covered under any other insurance providing health care benefits or services? |
|
||||||||||||||||||||
|
q Yes q No |
If “Yes”, please complete: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
a. Name of Policy Holder |
|
|
|
|
|
|
Relationship to Patient |
|
|
|
|
|
|
|
|
|
|||||
|
b. Name of Insuring Co. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
c. Policy or Certificate No. |
|
|
|
|
|
|
d. Effective Date of Coverage |
|
/ |
/ |
|
|
|
|
|
||||||
|
|
|
|
|
|
|
Month Day |
Year |
|
|||||||||||||
|
e. Check type of coverage: q Hospital |
q |
q Major Medical |
q Other (specify) |
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
f. Check One: I have |
q Family q Husband and Wife q Individual q Parent and Child coverage with this carrier. |
|
|||||||||||||||||||
|
g. Name and Address of Policy Holder’s Employer |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I certify the above is complete and correct and that I am claiming benefits only for charges incurred by the patient named above.
Any person who knowingly or willfully presents a false or fraudulent claim for payment of a loss or benefit or who knowingly or willfully presents false information in an application for insurance is guilty of a crime and may be subject to fines and confinement in prison.
Authorization is hereby given to any hospital, physician, or other provider which participated in any way in my care and treatment to release to CareFirst BlueCross BlueShield any medical information which they in their judgement deem necessary to the adjudication of this claim.
X
SIGNATURE OF SUBSCRIBER |
DATE |
HAVE YOU ATTACHED YOUR ITEMIZED BILLS?
Administrative Use Only
Do not write in this space
Provider# |
|
Initials |
CareFirst BlueCross BlueShield is the business name of CareFirst of Maryland, Inc. and is an independent licensee of the Blue Cross and Blue Shield Association.
® Registered trademark of the Blue Cross and Blue Shield Association. ®’ Registered trademark of CareFirst of Maryland, Inc.

Mail Administrator
P.O. Box 14115
Lexington, KY
STATE OF MARYLAND EMPLOYEES HEALTH CLAIM FORM
This form is to be used only by members of the State Employees Health Plan to file PPO, POS and EPO claims. While participating providers will bill CareFirst BlueCross BlueShield for services rendered, you may have claims to file yourself if you see
• A copy of the bill on the provider’s letterhead stationary
IN ORDER FOR YOUR CLAIMS TO BE PROCESSED, THE FOLLOWING INFORMATION MUST BE SUBMITTED
The bill must include:
Provider’s full name, degree, address, phone # and CareFirst BlueCross BlueShield provider number if available.
Patient’s full name
Descriptions of each service or supply
Date of which each service was provided
The provider’s diagnosis, or patient’s chief complaint
The amount charged by the provider for each service provided
Bills in foreign language should be translated to English, foreign currency should be converted to American dollars
Original bills and receipts required for all services
Keep a copy of your bills and claim for your records
Provider’s signature is required
•A completed claim form. Please be sure to accurately complete all sections of the claim form. Always use one claim form per patient.
•When another insurance carrier (including Medicare) is paying your claim first, please submit a copy of their payment statement with your claim. These statements are sometimes called “Explanation of Benefits,” “Summary of Benefits,” “Explanation of Medicare Benefits.”
BILLS FOR THE FOLLOWING SERVICES SHOULD INCLUDE THIS ADDITIONAL INFORMATION
Office Visits: |
Type of visit (brief, intermediate, extended, etc.) |
Private Duty Nursing: |
Dates and shifts worked, amount charged for each shift, prescribing Doctor’s name and degree, |
|
and registration # of nurse. |
Durable Medical Equipment: |
Include the full purchase price of any rented equipment. A letter of medical necessity from your |
(wheelchair, respirator, oxygen, etc.) |
physician must be submitted with the claim. |
Type of |
|
Blood Charges: |
Include the number of pints received, charges for each, and the number of pints replaced by |
|
donors. Indicate whether bill is for whole blood, plasma or derivatives. |
General Anesthesia: |
The length of time (in minutes) the patient was under general anesthesia must appear on the bill. |
Accidental Injury Claims: |
Must indicate the date on which the accident occurred. |
Members of the Preferred Provider Option (PPO), Exclusive Provider Organization (EPO) and Point of Service (POS) – Note: Must have pre- authorization on file after the sixth visit for outpatient physical therapy, occupational therapy and after first visit for speech therapy. See your benefit booklet, section: Managed Care Authorization Program for more information.
CareFirst BlueCross BlueShield State of Maryland Member Service
Access our website at www.carefirst.com/statemd