Are you considering enrolling in a memorial care program? Memorial care provides an array of services that can help those who have lost a loved one, from grief counseling to providing funding for travel expenses. Figuring out if you are eligible for these services can be daunting and confusing. In this blog post, we'll provide you with the necessary information about how to apply for memorial care eligibility. We'll discuss the requirements, what documents need to be provided, and any other important details about filing out your form correctly so that you can get access to the services that you need during this difficult time in your life.
| Question | Answer |
|---|---|
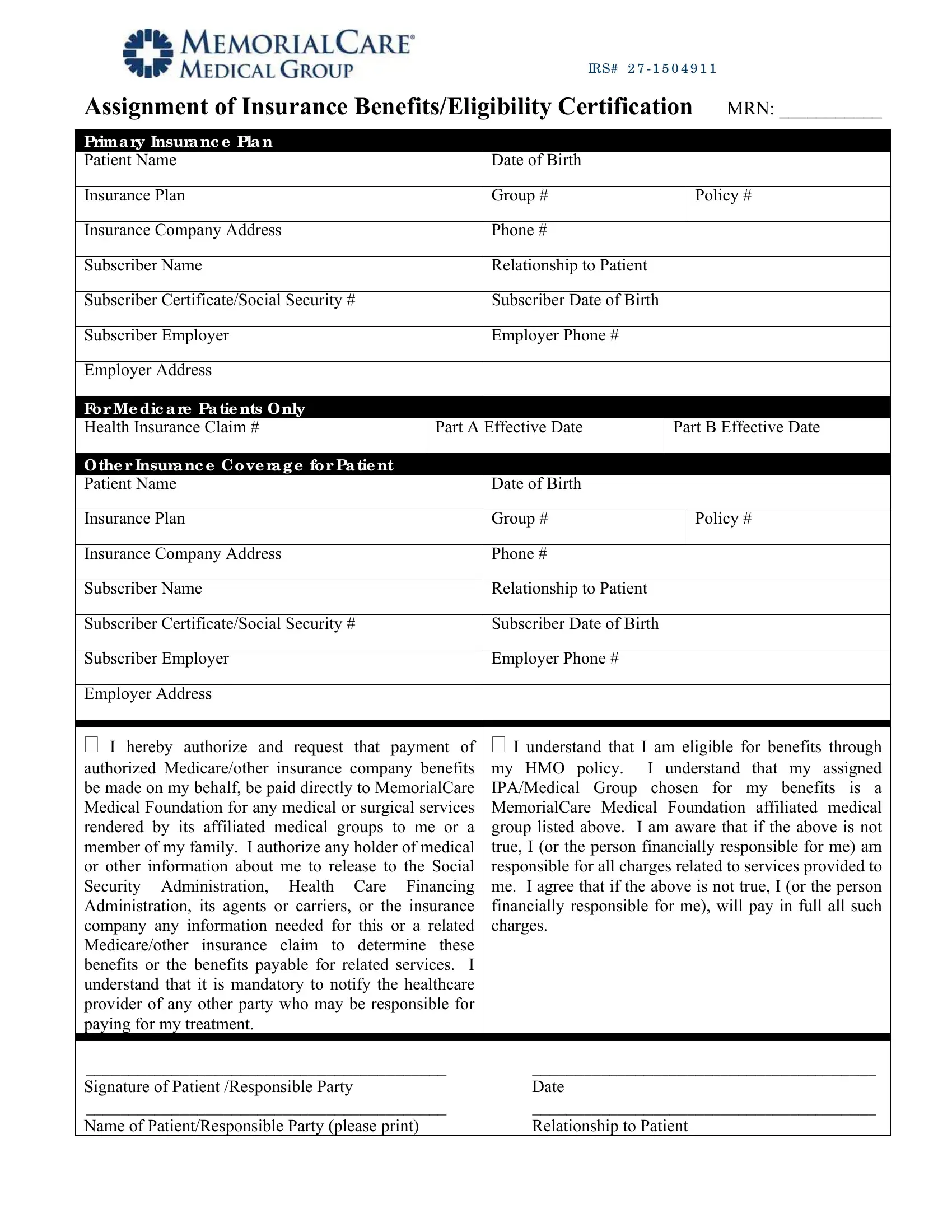
| Form Name | Memorial Care Eligibility Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | insurance eligibility verification, IRS, HMO, MRN |

IR S# 2 7 - 1 5 0 4 9 1 1
Assignment of Insurance Benefits/Eligibility Certification |
MRN: ___________ |
|||||
|
|
|
|
|
|
|
Prima ry Insura nc e Pla n |
|
|
|
|
|
|
Patient Name |
|
Date of Birth |
|
|
|
|
|
|
|
|
|
|
|
Insurance Plan |
|
Group # |
|
|
|
Policy # |
|
|
|
|
|
|
|
Insurance Company Address |
|
Phone # |
|
|
|
|
|
|
|
|
|
||
Subscriber Name |
|
Relationship to Patient |
|
|||
|
|
|
|
|
||
Subscriber Certificate/Social Security # |
|
Subscriber Date of Birth |
|
|||
|
|
|
|
|
|
|
Subscriber Employer |
|
Employer Phone # |
|
|
|
|
|
|
|
|
|
|
|
Employer Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
Fo r Me dic a re Pa tie nts O nly |
|
|
|
|
|
|
Health Insurance Claim # |
Part A Effective Date |
|
Part B Effective Date |
|||
|
|
|
|
|
|
|
O the r Insura nc e C o ve ra g e fo r Pa tie nt |
|
|
|
|
|
|
Patient Name |
|
Date of Birth |
|
|
|
|
|
|
|
|
|
|
|
Insurance Plan |
|
Group # |
|
|
|
Policy # |
|
|
|
|
|
|
|
Insurance Company Address |
|
Phone # |
|
|
|
|
|
|
|
|
|||
Subscriber Name |
|
Relationship to Patient |
|
|||
|
|
|
|
|||
Subscriber Certificate/Social Security # |
|
Subscriber Date of Birth |
|
|||
|
|
|
|
|
|
|
Subscriber Employer |
|
Employer Phone # |
|
|
|
|
|
|
|
|
|
|
|
Employer Address |
|
|
|
|
|
|
|
|
|||||
|
|
|||||
I hereby authorize and request that payment of |
I understand that I am eligible for benefits through |
|||||
authorized Medicare/other insurance company benefits |
my HMO policy. |
I understand that my assigned |
||||
be made on my behalf, be paid directly to MemorialCare |
IPA/Medical Group chosen for my benefits is a |
|||||
Medical Foundation for any medical or surgical services |
MemorialCare Medical Foundation affiliated medical |
|||||
rendered by its affiliated medical groups to me or a |
group listed above. |
I am aware that if the above is not |
||||
member of my family. I authorize any holder of medical |
true, I (or the person financially responsible for me) am |
|||||
or other information about me to release to the Social |
responsible for all charges related to services provided to |
|||||
Security Administration, Health Care Financing |
me. I agree that if the above is not true, I (or the person |
|||||
Administration, its agents or carriers, or the insurance |
financially responsible for me), will pay in full all such |
|||||
company any information needed for this or a related |
charges. |
|
|
|
|
|
Medicare/other insurance claim to determine these |
|
|
|
|
|
|
benefits or the benefits payable for related services. I |
|
|
|
|
|
|
understand that it is mandatory to notify the healthcare |
|
|
|
|
|
|
provider of any other party who may be responsible for |
|
|
|
|
|
|
paying for my treatment. |
|
|
|
|
|
|
|
|
|||||
__________________________________________ |
________________________________________ |
|||||
Signature of Patient /Responsible Party |
|
Date |
|
|
|
|
__________________________________________ |
________________________________________ |
|||||
Name of Patient/Responsible Party (please print) |
|
Relationship to Patient |
|
|||