If you are a Michigan resident who is looking to take advantage of their state’s medical marijuana laws, then the DCH-0654 form will be important for you. This form is necessary for anyone applying for a Medical Marihuana Program (MMP) card in the state of Michigan, and allows licensed physicians or certified nurse practitioners with prescriptive authority to issue certification of an individual's debilitating medical condition which makes them eligible to participate in the MMP program. Understanding what this form entails and making sure that it is completed properly can be essential to successfully obtaining your MMJ card. In this blog post, we'll discuss everything there is to know about the form – from eligibility requirements and filing deadlines to helpful resources and tips on completing the form correctly.
| Question | Answer |
|---|---|
| Form Name | Michigan Form Dch 0654 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | Dch 0654_66064_7 michigan lead abatement form dch 0654 |
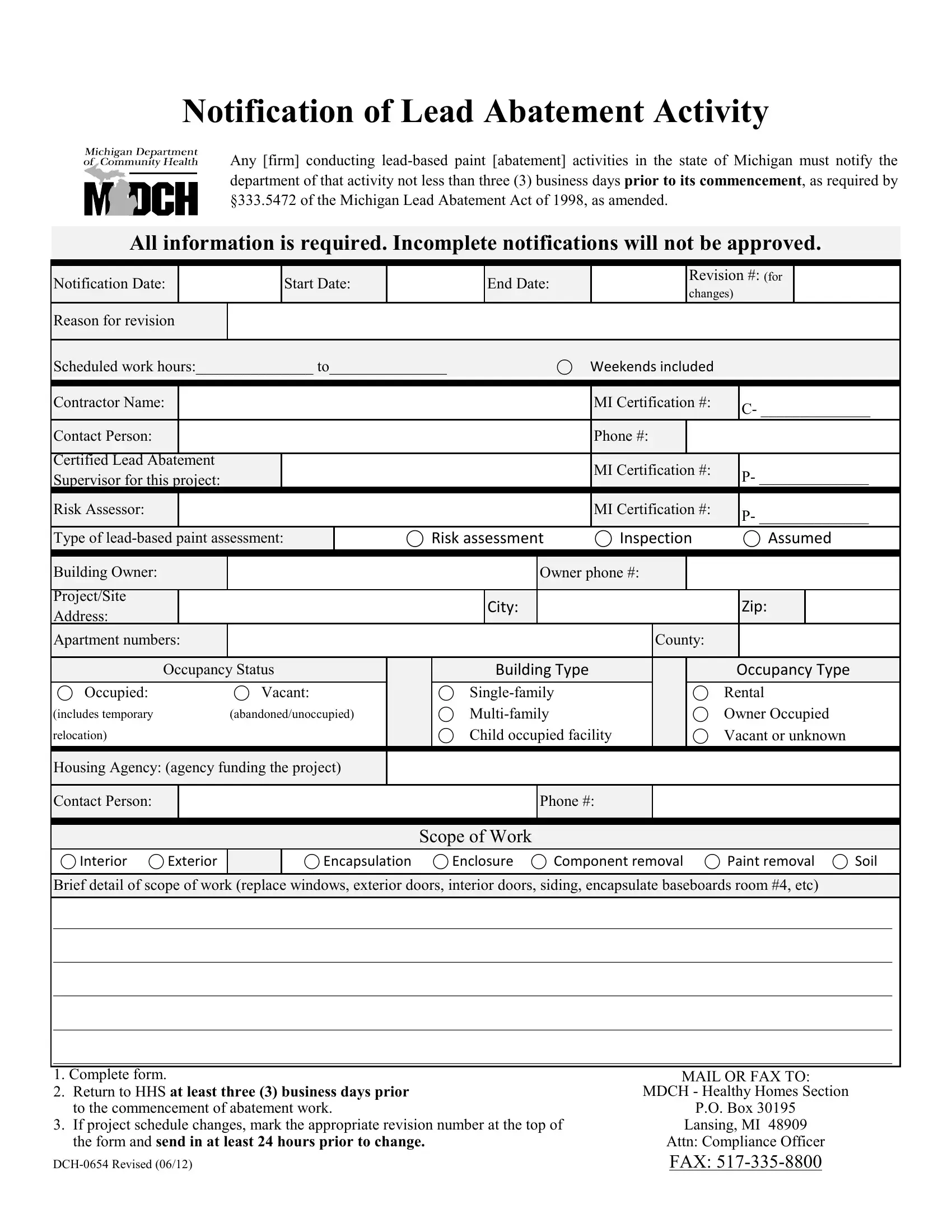
Notification of Lead Abatement Activity
Any [firm] conducting
All information is required. Incomplete notifications will not be approved.
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Notification Date: |
|
|
Start Date: |
|
|
End Date: |
|
|
|
Revision #: (for |
|
|
||||
|
|
|
|
|
|
|
changes) |
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Reason for revision |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Scheduled work hours:_______________ to_______________ |
⃝ |
Weekends included |
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Contractor Name: |
|
|
|
|
|
|
|
|
|
MI Certification #: |
C- ______________ |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Contact Person: |
|
|
|
|
|
|
|
|
|
Phone #: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Certified Lead Abatement |
|
|
|
|
|
|
|
|
MI Certification #: |
|
|
|
||||
Supervisor for this project: |
|
|
|
|
|
|
|
|
P- ______________ |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Risk Assessor: |
|
|
|
|
|
|
|
|
|
MI Certification #: |
P- ______________ |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Type of |
|
⃝ Risk assessment |
|
⃝ Inspection |
|
⃝ Assumed |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Building Owner: |
|
|
|
|
|
|
Owner phone #: |
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Project/Site |
|
|
|
|
|
|
City: |
|
|
|
|
|
|
Zip: |
|
|
Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Apartment numbers: |
|
|
|
|
|
|
|
|
|
County: |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Occupancy Status |
|
|
Building Type |
|
|
|
|
Occupancy Type |
||||||||
⃝ Occupied: |
⃝ Vacant: |
|
⃝ |
|
|
|
|
⃝ Rental |
||||||||
(includes temporary |
(abandoned/unoccupied) |
|
⃝ |
|
|
|
|
⃝ Owner Occupied |
||||||||
relocation) |
|
|
|
|
⃝ Child occupied facility |
|
|
⃝ Vacant or unknown |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Housing Agency: (agency funding the project)
Contact Person:
Phone #:
Scope of Work
⃝ Interior ⃝ Exterior
⃝ Encapsulation ⃝ Enclosure ⃝ Component removal ⃝ Paint removal ⃝ Soil
Brief detail of scope of work (replace windows, exterior doors, interior doors, siding, encapsulate baseboards room #4, etc)
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
1. Complete form.
2. Return to HHS at least three (3) business days prior to the commencement of abatement work.
3. If project schedule changes, mark the appropriate revision number at the top of the form and send in at least 24 hours prior to change.