Are you a Missouri resident looking to file your taxes this year? Knowing which forms to fill out and when can be complicated, so having the right information is essential. To ensure that you are up-to-date on all the deadlines and details, it's important to understand what exactly Missouri Form CD 147 is and how it relates to tax filing season. Read on for an overview of everything you need to know about Missouri Form CD 147, including what it’s used for, who needs to use it, when it’s due, and how to submit your form correctly.
| Question | Answer |
|---|---|
| Form Name | Missouri Form Cd 147 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | LINC, legibly, fillable cd 147, MISSOURI |
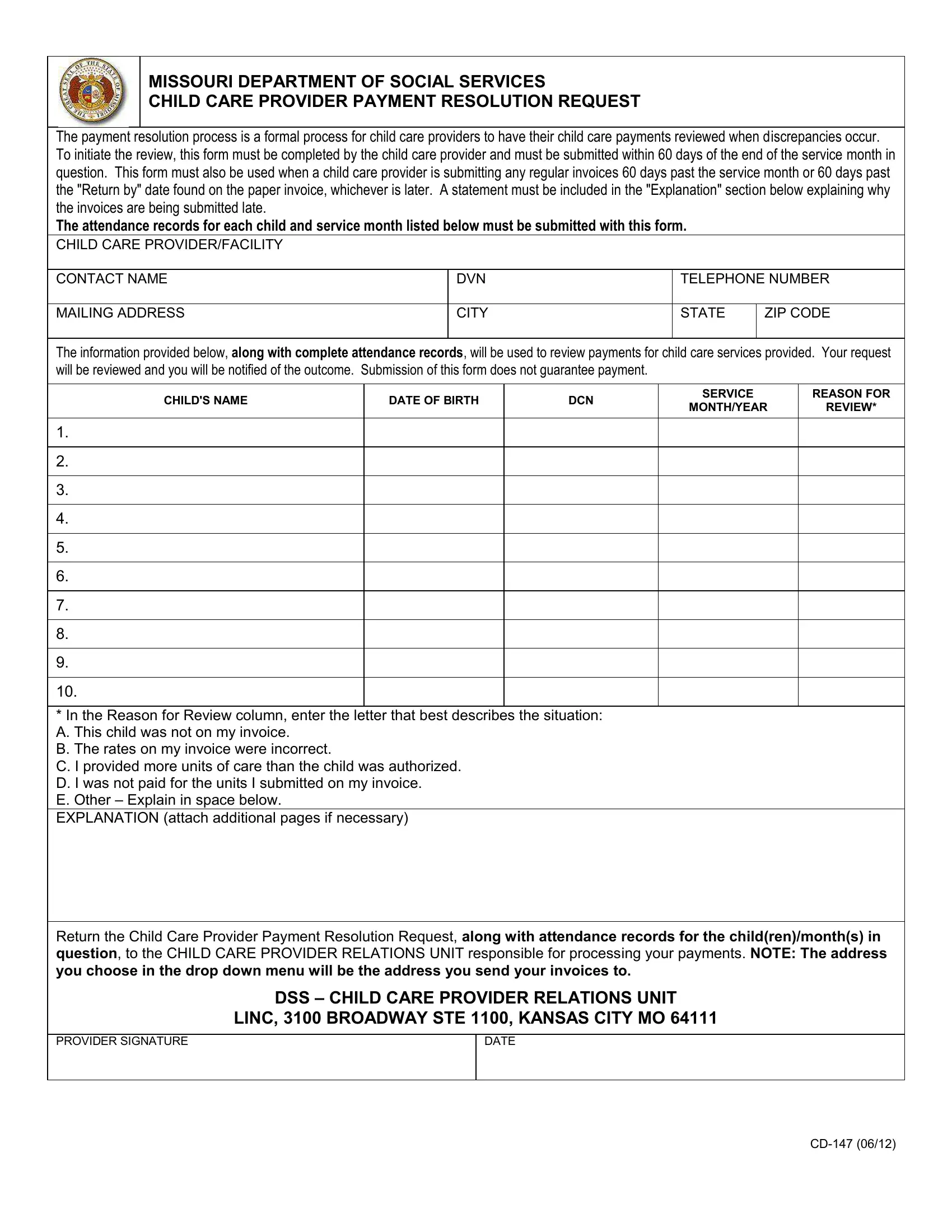
MISSOURI DEPARTMENT OF SOCIAL SERVICES
CHILD CARE PROVIDER PAYMENT RESOLUTION REQUEST
The payment resolution process is a formal process for child care providers to have their child care payments reviewed when discrepancies occur. To initiate the review, this form must be completed by the child care provider and must be submitted within 60 days of the end of the service month in question. This form must also be used when a child care provider is submitting any regular invoices 60 days past the service month or 60 days past the "Return by" date found on the paper invoice, whichever is later. A statement must be included in the "Explanation" section below explaining why the invoices are being submitted late.
The attendance records for each child and service month listed below must be submitted with this form.
CHILD CARE PROVIDER/FACILITY
CONTACT NAME
DVN
TELEPHONE NUMBER
MAILING ADDRESS
CITY
STATE
ZIP CODE
The information provided below, along with complete attendance records, will be used to review payments for child care services provided. Your request will be reviewed and you will be notified of the outcome. Submission of this form does not guarantee payment.
CHILD'S NAME |
DATE OF BIRTH |
DCN |
SERVICE |
REASON FOR |
|
MONTH/YEAR |
REVIEW* |
||||
|
|
|
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
*In the Reason for Review column, enter the letter that best describes the situation: A. This child was not on my invoice.
B. The rates on my invoice were incorrect.
C. I provided more units of care than the child was authorized.
D. I was not paid for the units I submitted on my invoice. E. Other – Explain in space below.
EXPLANATION (attach additional pages if necessary)
Return the Child Care Provider Payment Resolution Request, along with attendance records for the child(ren)/month(s) in question, to the CHILD CARE PROVIDER RELATIONS UNIT responsible for processing your payments. NOTE: The address you choose in the drop down menu will be the address you send your invoices to.
DSS – CHILD CARE PROVIDER RELATIONS UNIT
LINC, 3100 BROADWAY STE 1100, KANSAS CITY MO 64111
PROVIDER SIGNATURE
DATE
CHILD CARE PROVIDER PAYMENT RESOLUTION REQUEST
PURPOSE:
The Child Care Provider Payment Resolution Request is the form providers are required to submit when payments need to be reviewed for discrepancies. Submitting the Child Care Provider Payment Resolution Request will initiate the process for payments to be reviewed for discrepancies.
INSTRUCTIONS:
This form may be typed or legibly handwritten by the child care provider or a representative of the child care provider.
To be eligible for review, all Child Care Provider Payment Resolution Request forms must be submitted with complete attendance records for each child and service month in question.
CHILD CARE PROVIDER/FACILITY - Enter the child care facility name or the child care provider's name.
CONTACT NAME - Enter the name of the person that can be contacted for any questions pertaining to the resolution request.
DVN - Enter the Departmental Vendor Number (DVN) for the facility or the provider.
TELEPHONE NUMBER - Enter the telephone number of the contact name.
MAILING ADDRESS - Enter the mailing address of the facility or individual child care provider.
CITY - Enter the city for the mailing address of the facility or individual child care provider.
STATE - Enter the state for the mailing address of the facility or individual child care provider.
ZIP CODE - Enter the zip code for the mailing address of the facility or individual child care provider.
CHILD'S NAME - Enter the child's name for which payment review is being requested. Each form allows up to ten children to be listed for payment review.
DATE OF BIRTH - Enter the child's date of birth for which payment review is being requested.
DCN - Enter the child's DCN for which payment review is being requested. A dcn will need to be entered for each individual child listed.
SERVICE MONTH/YEAR - Enter the service month and year for which payment review is being requested.
REASON FOR REVIEW - Enter the letter (A – E) corresponding to the reason for the review request. (The different reasons are listed below the child's name listing 1 – 10.)
EXPLANATION - Enter any information that may support the request for review.
RETURN THE CHILD CARE PROVIDER PAYMENT REQUEST
Go to the drop down box beside the DSS – Child Care Provider Relations Unit and select the address of the Provider Relations Unit responsible for processing your payments. The address you select in the drop down menu should be the address you send your invoices to.
OAddresses you can choose from to send your payment resolution request to:
PO Box 88, Jefferson City, MO,
LINC, 3100 Broadway, Ste 1100, Kansas City, MO, 64111
4411 N Newstead Ave, 3rd Fl, St. Louis, MO, 63115
PROVIDER SIGNATURE - You must sign the request and keep a copy for your records.
DATE
Enter the date of the request.
Once the Child Care Provider Payment Resolution Request has been completed in full, the provider will attach the appropriate attendance record(s) and mail the request to the DSS – Child Care Provider Relations Unit with the address selected from the drop down menu. Provider must keep a copy of the requests and attendance records for their records. Attendance records will not be returned.