Are you enrolled in Medicaid and need to know how to get your credit balance report? Then read on for all the info you need! The Nc Medicaid Credit Balance Report Form is an important document in managing and tracking any/all of a Medicaid beneficiary’s financial transactions. It helps to ensure that beneficiaries have accurate information available when filing claims or making payments, while also providing clinicians with up-to-date account statements of their client’s accounts. This post will go over the how's and why's of the Nc Medicaid Credit Balance Report Form and what it entails so that you can be better informed about this critical yet often overlooked part of managing one’s finances.
| Question | Answer |
|---|---|
| Form Name | Nc Medicaid Credit Balance Report Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | ICN, medicaid credit balance report, Raleigh, nc medicaid credit balance report |
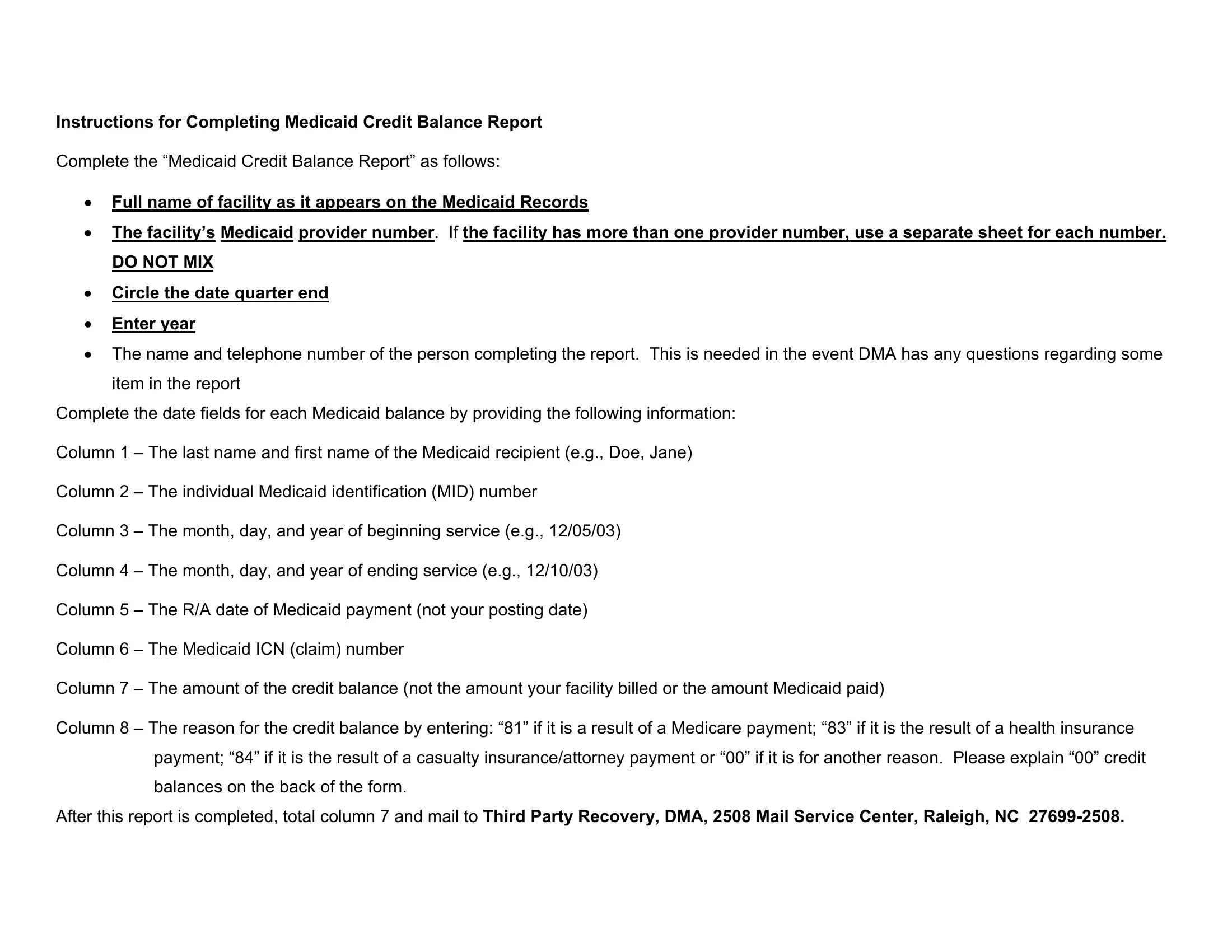
Instructions for Completing Medicaid Credit Balance Report
Complete the “Medicaid Credit Balance Report” as follows:
•Full name of facility as it appears on the Medicaid Records
•The facility’s Medicaid provider number. If the facility has more than one provider number, use a separate sheet for each number.
DO NOT MIX
•Circle the date quarter end
•Enter year
•The name and telephone number of the person completing the report. This is needed in the event DMA has any questions regarding some
item in the report
Complete the date fields for each Medicaid balance by providing the following information:
Column 1 – The last name and first name of the Medicaid recipient (e.g., Doe, Jane)
Column 2 – The individual Medicaid identification (MID) number
Column 3 – The month, day, and year of beginning service (e.g., 12/05/03)
Column 4 – The month, day, and year of ending service (e.g., 12/10/03)
Column 5 – The R/A date of Medicaid payment (not your posting date)
Column 6 – The Medicaid ICN (claim) number
Column 7 – The amount of the credit balance (not the amount your facility billed or the amount Medicaid paid)
Column 8 – The reason for the credit balance by entering: “81” if it is a result of a Medicare payment; “83” if it is the result of a health insurance payment; “84” if it is the result of a casualty insurance/attorney payment or “00” if it is for another reason. Please explain “00” credit balances on the back of the form.
After this report is completed, total column 7 and mail to Third Party Recovery, DMA, 2508 Mail Service Center, Raleigh, NC
MEDICAID CREDIT BALANCE REPORT
PROVIDER NAME:__________________________ CONTACT PERSON: ___________________________________
PROVIDER NUMBER: _______________________ TELEPHONE NUMBER: _________________________________
QUARTER ENDING: (Circle one) 3/31 6/30 |
9/30 12/31 |
YEAR: _________________ |
|
|
|||
(1) |
(2) |
(3) |
(4) |
(5) |
(6) |
(7) |
(8) |
RECIPIENT’S |
MEDICAID |
FROM DATE |
TO DATE |
DATE |
MEDICAID |
AMOUNT OF |
REASON |
NAME |
NUMBER |
OF |
OF SERVICE |
MEDICAID |
ICN |
CREDIT |
FOR CREDIT |
|
|
SERVICE |
|
PAID |
|
BALANCE |
BALANCE |
|
|
|
|
|
|
|
|
1. |
|
|
|
|
|
|
|
2. |
|
|
|
|
|
|
|
3. |
|
|
|
|
|
|
|
4. |
|
|
|
|
|
|
|
5. |
|
|
|
|
|
|
|
6. |
|
|
|
|
|
|
|
7. |
|
|
|
|
|
|
|
8. |
|
|
|
|
|
|
|
9. |
|
|
|
|
|
|
|
10. |
|
|
|
|
|
|
|
11. |
|
|
|
|
|
|
|
12. |
|
|
|
|
|
|
|
13. |
|
|
|
|
|
|
|
14. |
|
|
|
|
|
|
|
15. |
|
|
|
|
|
|
|
Circle one: |
Refund |
Adjustment |
|
|
Return form to: |
Third Party Recovery |
|
|
|
|
|
|
|
DMA |
|
2508 Mail Service Center
Raleigh, NC
Revised 10/07