Are you looking for an easier way to help your child receive State Aid funds? Filling out the necessary forms can be complicated and overwhelming. That’s why we have created this guide – to give you the information you need about filing for the New York State Aid Voucher form. Here, we provide a step-by-step review of all essential guidelines and instructions needed when applying for this voucher program. We believe that everyone should have access to financial assistance when it is needed most, so read on to find out how to file your application today!
| Question | Answer |
|---|---|
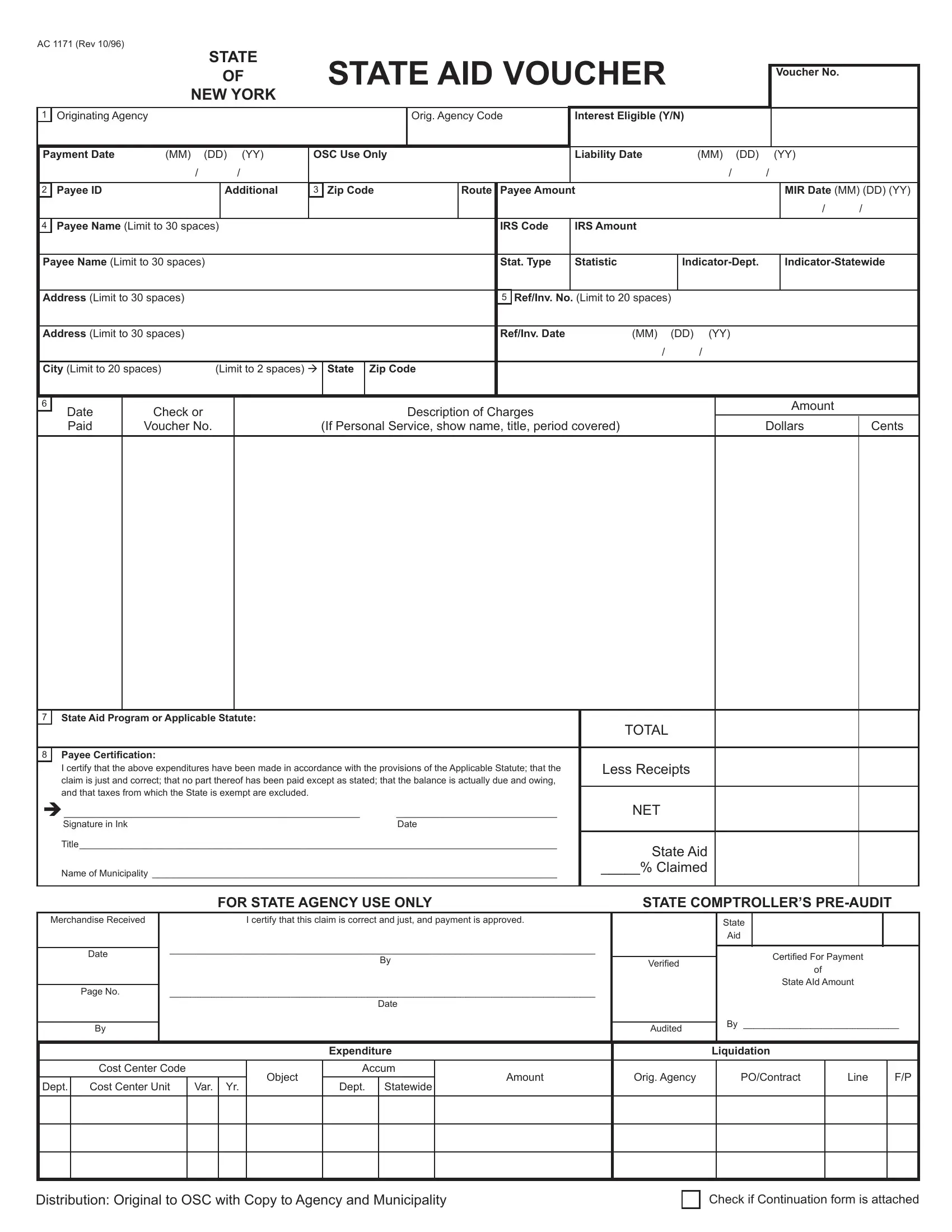
| Form Name | Nys State Aid Voucher Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | ac 1171 rev 3 2002, state aid voucher fillable, state of new york state aid voucher form, aid voucher get |

AC 1171 (Rev 10/96)
STATE
OF STATE AID VOUCHER
NEW YORK
Voucher No.
1 |
Originating Agency |
|
|
|
|
|
|
Orig. Agency Code |
Interest Eligible (Y/N) |
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Payment Date |
(MM) |
(DD) (YY) |
OSC Use Only |
|
|
|
|
Liability Date |
|
(MM) (DD) |
|
(YY) |
|
|||||||
|
|
/ |
/ |
|
|
|
|
|
|
|
|
/ |
/ |
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
Payee ID |
|
|
Additional |
3 Zip Code |
|
Route |
Payee Amount |
|
|
|
|
|
MIR Date (MM) (DD) (YY) |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 |
Payee Name (Limit to 30 spaces) |
|
|
|
|
|
IRS Code |
IRS Amount |
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Payee Name (Limit to 30 spaces) |
|
|
|
|
|
Stat. Type |
Statistic |
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Address (Limit to 30 spaces) |
|
|
|
|
|
|
|
|
5 |
Ref/Inv. No. (Limit to 20 spaces) |
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address (Limit to 30 spaces) |
|
|
|
|
|
|
|
|
Ref/Inv. Date |
(MM) |
(DD) (YY) |
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City (Limit to 20 spaces) |
(Limit to 2 spaces) à |
State |
Zip Code |
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6 |
Date |
Check or |
|
|
|
|
|
|
Description of Charges |
|
|
|
|
|
|
Amount |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
Paid |
Voucher No. |
|
(If Personal Service, show name, title, period covered) |
|
|
|
Dollars |
Cents |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7State Aid Program or Applicable Statute:
TOTAL
8 |
Payee Certiication: |
|
|
|
|
I certify that the above expenditures have been made in accordance with the provisions of the Applicable Statute; that the |
|
Less Receipts |
|
|
claim is just and correct; that no part thereof has been paid except as stated; that the balance is actually due and owing, |
|
|
|
|
and that taxes from which the State is exempt are excluded. |
|
|
|
è_________________________________________________________ |
_______________________________ |
|
NET |
|
|
Signature in Ink |
Date |
|
|
|
Title____________________________________________________________________________________________ |
|
State Aid |
|
|
|
|
|
|
|
Name of Municipality ______________________________________________________________________________ |
|
_____% Claimed |
|
|
|
|
||
|
|
|
|
|
|
FOR STATE AGENCY USE ONLY |
|
STATE COMPTROLLER’S |
|
Merchandise Received
Date
Page No.
By
I certify that this claim is correct and just, and payment is approved.
__________________________________________________________________________________
By
__________________________________________________________________________________
Date
Veriied
Audited
State
Aid
Certiied For Payment
of
State AId Amount
By ______________________________
|
|
|
|
|
Expenditure |
|
|
Liquidation |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cost Center Code |
|
|
Object |
Accum |
Amount |
Orig. Agency |
|
PO/Contract |
Line |
F/P |
|
Dept. |
Cost Center Unit |
Var. |
Yr. |
Dept. |
Statewide |
|
||||||
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Distribution: Original to OSC with Copy to Agency and Municipality
Check if Continuation form is attached