Are you an individual or business owner looking for information on how to fill out and submit the OMB form 1510? If so, then this blog post is perfect for you! In it, we will provide a detailed overview of what the Omb Form 1510 is, what its purpose is, and how to properly complete it. We will explain each section clearly and include tips on making sure nothing gets missed during submission. With our guidance in hand, submitting your form should be quick and painless - let's get started!
| Question | Answer |
|---|---|
| Form Name | Omb Form 1510 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | 11_ACHOMBForm15 10 fws ach form 2011 |
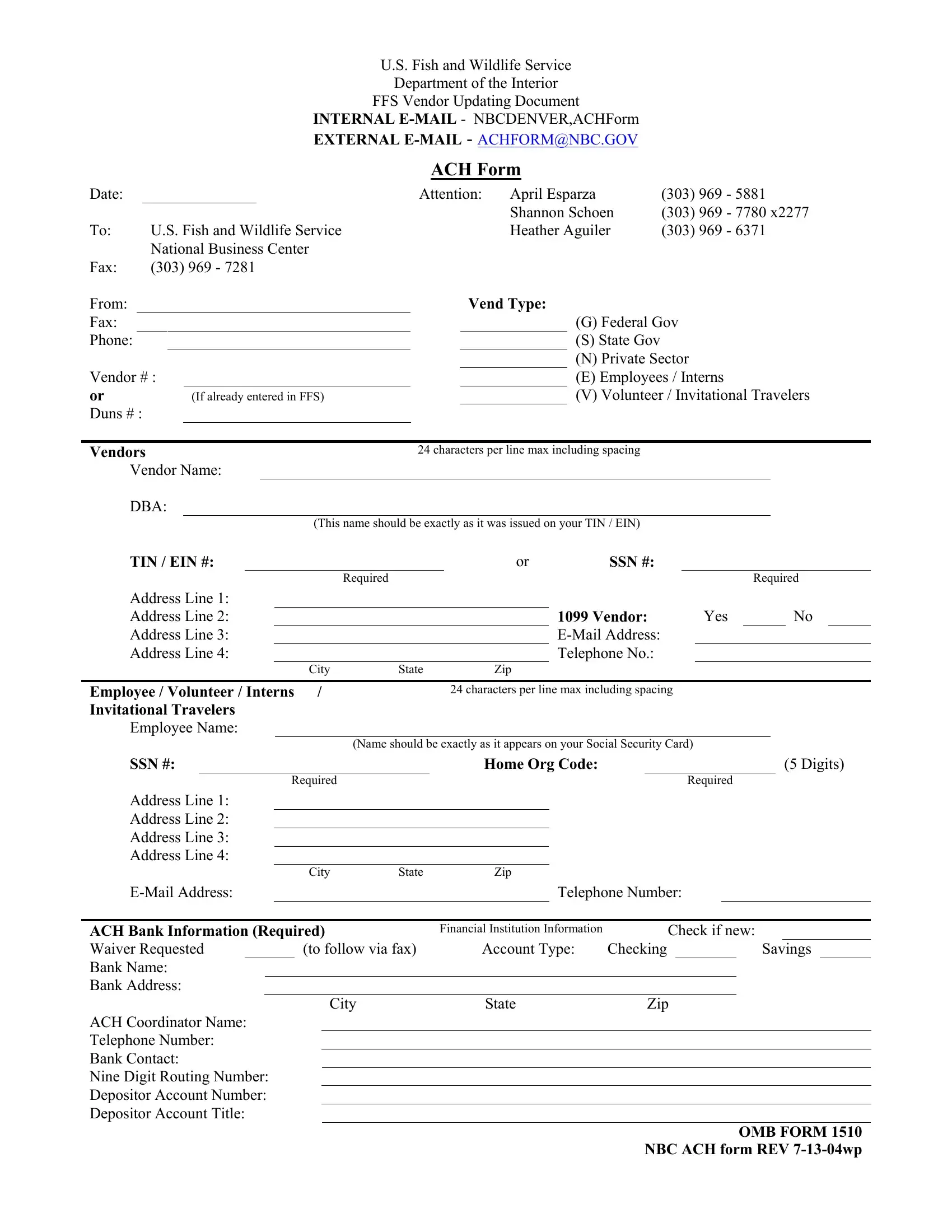
U.S. Fish and Wildlife Service
Department of the Interior
FFS Vendor Updating Document
INTERNAL
EXTERNAL
ACH Form
Date: |
|
Attention: |
April Esparza |
(303) 969 - 5881 |
|
|
|
|
Shannon Schoen |
(303) 969 |
- 7780 x2277 |
To: |
U.S. Fish and Wildlife Service |
Heather Aguiler |
(303) 969 |
- 6371 |
|
|
National Business Center |
|
|
|
|
Fax: |
(303) 969 - 7281 |
|
|
|
|
From:
Fax:
Phone:
Vendor # :
or |
(If already entered in FFS) |
Duns # : |
|
Vend Type:
(G)Federal Gov
(S)State Gov
(N)Private Sector
(E) Employees / Interns
(V) Volunteer / Invitational Travelers
Vendors |
24 characters per line max including spacing |
||
Vendor Name: |
|
|
|
DBA: |
|
|
|
|
(This name should be exactly as it was issued on your TIN / EIN) |
||
TIN / EIN #: |
|
or |
SSN #: |
|
Required |
|
|
Required
Address Line 1: |
|
|
|
|
|
|
Address Line 2: |
|
1099 Vendor: |
Yes |
|
No |
|
Address Line 3: |
|
|
|
|
|
|
Address Line 4: |
|
Telephone No.: |
|
|
|
|
City |
State |
Zip |
|
|
|
Employee / Volunteer / Interns / |
|
24 characters per line max including spacing |
Invitational Travelers
Employee Name:
(Name should be exactly as it appears on your Social Security Card)
SSN #: |
Home Org Code: |
Required
(5 Digits)
Required
Address Line 1:
Address Line 2:
Address Line 3:
Address Line 4:
|
City |
State |
Zip |
|
|
|
|
Telephone Number: |
|
ACH Bank Information (Required)
Waiver Requested (to follow via fax) Bank Name:
Bank Address:
Financial Institution Information |
|
Check if new: |
|
|||
Account Type: |
Checking |
|
|
Savings |
|
|
City |
State |
Zip |
ACH Coordinator Name:
Telephone Number:
Bank Contact:
Nine Digit Routing Number:
Depositor Account Number:
Depositor Account Title:
OMB FORM 1510
NBC ACH form REV