
When working in the online tool for PDF editing by FormsPal, you'll be able to complete or change forms 522 here. Our editor is continually evolving to provide the best user experience attainable, and that is thanks to our commitment to continuous improvement and listening closely to feedback from users. If you're looking to start, here is what it will require:
Step 1: First of all, open the pdf tool by clicking the "Get Form Button" above on this site.
Step 2: The editor lets you customize most PDF documents in a variety of ways. Change it with any text, correct existing content, and put in a signature - all doable within minutes!
With regards to the blank fields of this specific form, here is what you should do:
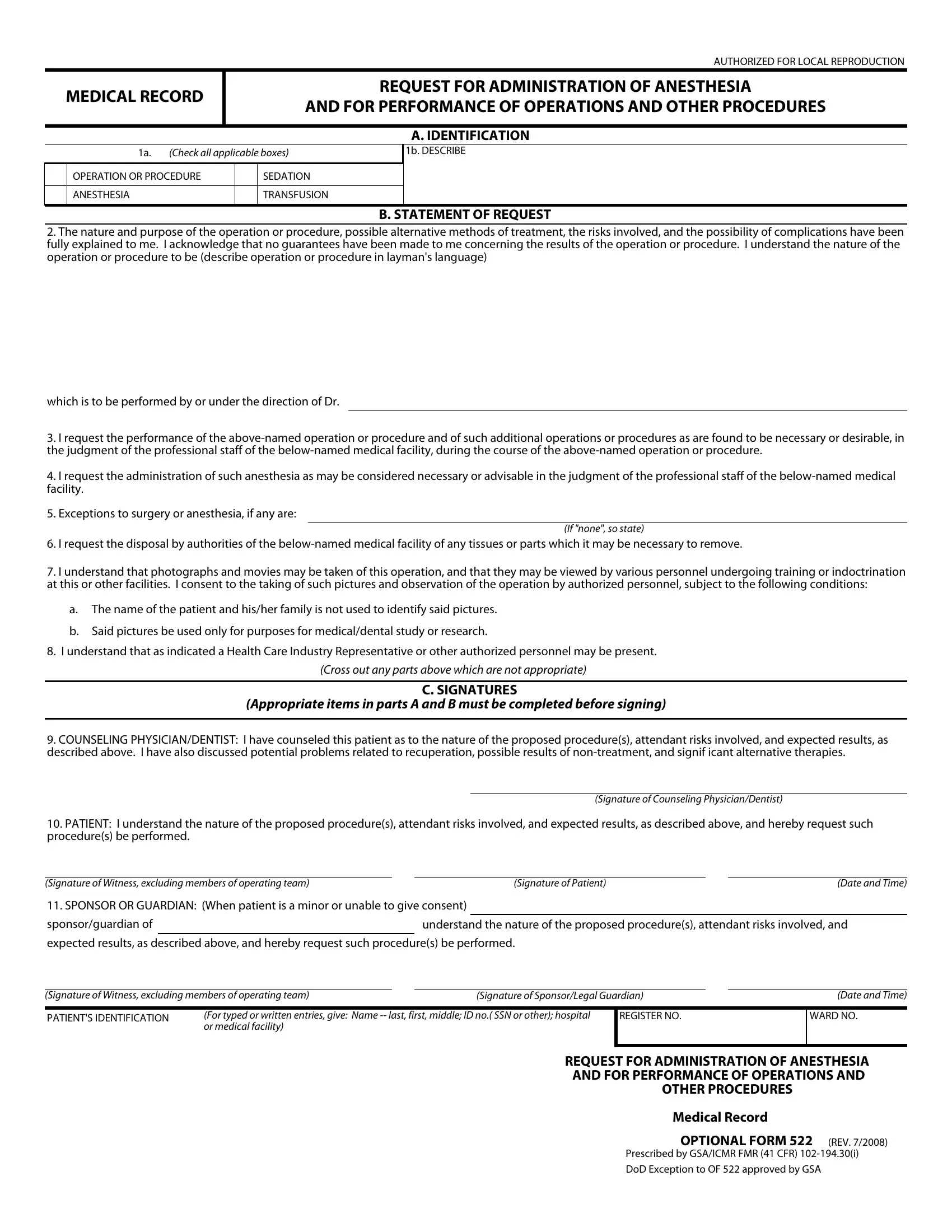
1. Begin completing your forms 522 with a selection of essential blank fields. Collect all of the required information and ensure not a single thing missed!
2. Soon after finishing this section, head on to the next step and complete the necessary details in these blanks - PATIENT I understand the nature, Signature of Witness excluding, Signature of Patient, Date and Time, SPONSOR OR GUARDIAN When patient, sponsorguardian of, understand the nature of the, expected results as described, Signature of Witness excluding, Signature of SponsorLegal Guardian, PATIENTS IDENTIFICATION, For typed or written entries give, REGISTER NO, Date and Time, and WARD NO.
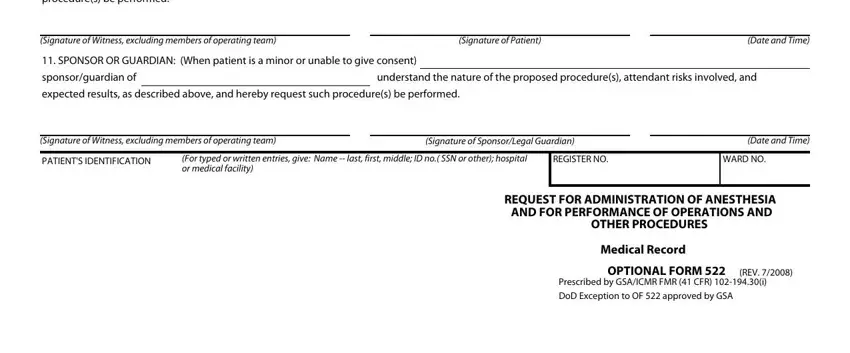
Be really attentive when completing REGISTER NO and understand the nature of the, because this is the part where most people make errors.
Step 3: As soon as you have looked over the information provided, click on "Done" to complete your form. Try a 7-day free trial subscription at FormsPal and get direct access to forms 522 - download, email, or edit from your personal cabinet. Whenever you work with FormsPal, it is simple to fill out forms without being concerned about personal data breaches or entries getting distributed. Our protected software ensures that your private data is kept safely.